

I'm not against patients using cannabis if it helps, but the science isn't strong.
This article is going to discuss medicinal cannabis.
This has been a bit of a vexed issue over time in my rheumatology practice. Patients I had in the drug squad told me they didn’t care about personal use of cannabis, so I often recommended patients get some seeds from their grandchildren and see if this helped (preferably as butter rather than smoked).
This was put to the test when the police rang me and asked if I had made this recommendation for a specific patient. I said yes and they then asked if I told to her to grow 57 plants! Clearly this was a bit excessive but there was no evidence she was selling it, so she got off with a caution (but she probably should have been offered a job as a gardening consultant).
Generally, it seemed to help when it was used in this way. Now it is legal (but expensive), I have had a lot more experience. Results range from amazing to absolutely nothing, with more of the latter. It seems to be a best fit for fibromyalgia but the published evidence is based on two small trials using inhaled cannabis. The distinctive smell makes it impossible to blind thus these trials are suspect as well as short term. It doesn’t seem to do much for osteoarthritis and clearly we have better options for inflammatory arthritis.
There have been some reviews studying a potpourri of conditions, with none specifically within our area. These have generally had small numbers. Thus, it was a surprise to see how many trials there were if you tried to use all the data as in the recent paper by Wang et al. (including our own Rachelle Buchbinder).
This overview used rigorous Cochrane methodology. There were 32 trials with more than 5,000 subjects. It was still a real mix of subjects with neuropathic being the most common (11 trials) but cancer and headache were also included. They included only studies lasting more than four weeks and which included oral, sublingual or topical (no inhaled). You can take the simple approach by looking at the forest plot below and concluding that cannabis was modestly effective for pain with WMD (weighted mean difference) -0.63 (as well as sleep and physical functioning).
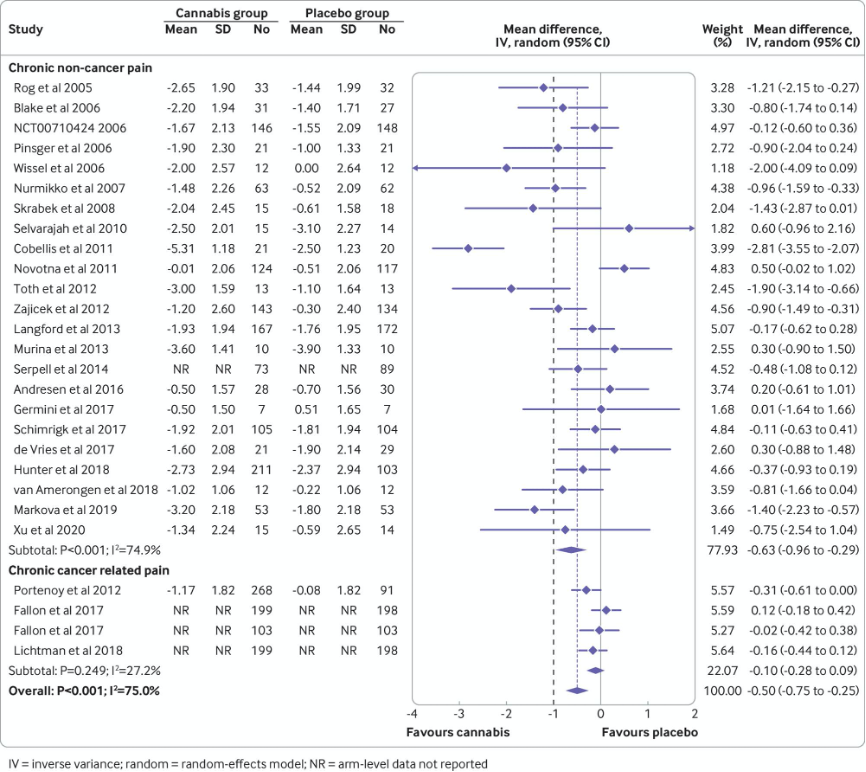
However, my view is that this would be wrong. From the figure, you can see results are heterogeneous (as many of the confidence limits don’t overlap). Also, the larger trials tend to have smaller or non-significant effects, suggesting bias in the smaller trials (even if the authors didn’t document this in a formal meta-regression). There are even five trials that are numerically worse than placebo (which is quite rare in my experience).
Overall, there was a high risk of bias in these studies. The supplementary tables did suggest that it works better in non-cancer pain and specifically non-neuropathic pain. It also suggested the combination of tetrahydrocannabinol (THC) and cannabidiol (CBD) works better than CBD alone and this has issues for drug testing. I have tended to used CBD alone for this reason but may need to rethink this.




There was also some modest toxicity with transient cognitive impairment, vomiting, drowsiness, impaired attention, nausea and dizziness. Oral had more dizziness than topical; otherwise, they seemed similar.
When you combine my recent experience with the lack of studies in our area and the modest efficacy and toxicity in other areas, I remain a bit uncertain about whether cannabis really does have a place in the rheumatology armamentarium. What I would like is a well-done trial in fibromyalgia (and maybe osteoarthritis) with adequate blinding before I become more (or less) enthusiastic.
I also need some high-quality data on which of the more than 140 active components help therapeutically. I was involved in designing one of these studies a number of years ago with Australian companies but there has been no progress, as far as I am aware.
Graeme Jones is Professor of Rheumatology and Epidemiology and Head of the Musculoskeletal Unit at the Menzies Institute for Medical Research
