
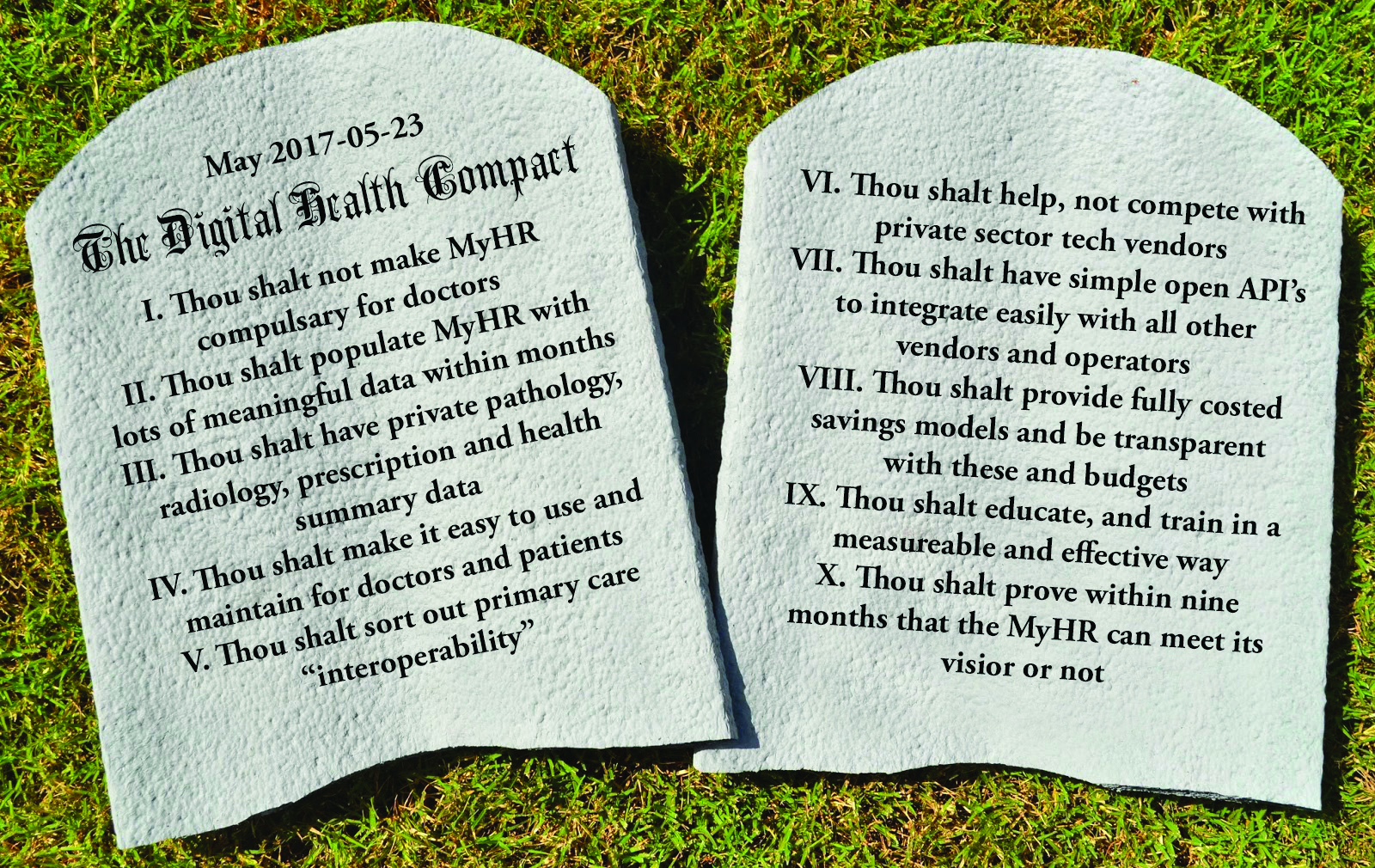
Here it is. The MyHR ADHA compact between the healthcare sector and the Australian people that we really need
The RACGP and AMA compacts with the federal government aren’t seen by most GPs as meaningful, which isn’t surprising. At just 55c extra per consult this coming year, a drawn-out path to a full lift of the freeze over the following two years, and not much else, these contracts were always at risk of being seen as limp. The agreements might in fact be locking in a position of no progress, or worse, ongoing regression. After all, we’ve now firmly agreed to snail’s pace changes to MBS rebates, which essentially keep GPs well under any sort of indexed pay rise for the next few years. And that’s the tangible part of this compact.
As much as the RACGP has led with its chin by making such a compact, blaming the College is probably a little simplistic. They are, after all, mainly a training organisation. Plus, they’ve grown into an organisation that is large and struggling to undersand what it is. As such it is a little unwieldy in terms of governance and leadership in matters like these. Which is a long way of saying, the College at this point really isn’t set up for this sort of stuff.
The AMA is largely an employment and lobbying organisation, so perhaps we could blame them a little more, but as with the RACGP, navigating the politics of such big organisations tends to dilute the ability to lead change.
So is there any hope of transformative change for general practice in the near future?
There might be. But from the most unlikely of places. Perhaps from a place that has been moribund for so long it has entered mythology as one of greatest government screw-ups of all time. From the agency that brings us – I’m almost reluctant to mention the name here lest you stop reading or fall asleep in your chair – the My Health Record. Yes, the Australian Digital Health Agency, previously NEHTA.
Before you click away, or flip the page, bear with me for just a second. The federal government didn’t get into the game of digital transformation just to make us all laugh, or cry, at how much they could screw things up so thoroughly. They had good intent. They just didn’t have a clue after that. Which doesn’t exactly excuse spending nearly $1.5 billion on trying to establish a nationwide digital health record for all Australians and four years on, having very little to show for it.
But just say you could make some form of the My Health Record meet some of its intended specifications sooner rather than later. Say you could make substantial progress towards this goal within the next nine months. What might that look for GPs and their patients?
Do not click away chuckling.
I’m suggesting it because the Australian Digital Health Agency (ADHA), the organisation now responsible for the MyHR, could, more or less, enter into a compact with the GP profession and the public right now – a compact that could deliver tangible and substantive progress within nine months. That’s not that long to wait, given what we’ve gone through so far.
Under this plan, if the ADHA didn’t deliver within the timeframe, they would have broken the compact, and we could all return to our exhausted and cynical corners, having wasted at least another $200m or so. And presumably, those in charge would fall on their respective swords.
Currently, I don’t agree with how much the ADHA and thus, the MyHR, is spending, and on what. But if the basics of this compact were realised, we would all see tangible progress towards potentially transformative change. Change that would effectively benefit patients and doctors, and even lead to increased GP incomes, well above what would be delivered under the RACGP and AMA compacts.
So here it is. The MyHR ADHA 10-point compact between the Australian healthcare sector and the Australian people, authored by me but with input from various sources, whether they know it or not.
No 1.
Despite recommendations in the recently released Siggins Miller report into the MyHR opt-out trials, the ADHA has no intention of trying to make the MyHR compulsory for healthcare professionals. Rather, they believe the MyHR will be used by all parts of the sector in the not too distant future, simply because it will be useful – it will save time, money and lives. Many will start to see this, be compelled to have a second look and try it.
No 2.
Significant and meaningful data will reside in the MyHR and will be apparent within the next few months. By nine months, there will be enough actual data for the MyHR to be very useful to patients and doctors alike.
“The federal government didn’t get into the game of digital transformation just to make us all laugh, or cry, at how much they could screw things up so thoroughly.”
No 3.
Such data will include but not be limited to:
a. Private pathology data, provided by all the major private pathology providers within the nine-month period. Until now, these parties have been noticeable absentees from the MyHR program. Getting them on board will provide a source of data that will immediately make the MyHR compelling. But perhaps more importantly, their joining the project might be symbolic of a coming together of previously disparrate and sometimes warring parties, for the greater good.
b. Prescribing data uploaded directly by community pharmacy through their POS and prescription management systems. This is particularly exciting because this is data is far more accurate and useful than previously available data on prescriptions. It has never been collated and available before as it will be in this project.
c. Meaningful health summaries created by GPs.
d. Automated loading of these summaries so GPs don’t waste their time acting as data entry clerks.
No 4.
That the user interface for both patients and health providers will be upgraded so that enrolling in the MyHR is much easier and ongoing participation is far more seamless. As much as is feasible, this process will be automated so that neither party will be unnecessarily burdened with data entry, but will benefit from the wonders of modern integrated data-sharing platforms, including the sharing of data, where authorised, through the cloud and in real time.
No 5.
The MyHR already talks to the all the major GP-based patient management systems but it will now also move into the realm of specialists via those systems and significantly improved interoperability between GP and specialists’ patient management systems. Progress in interoperability between various software, pathology, radiology and other vendors will see the fax era come to an end and open up previously inaccessible areas of healthcare delivery like specialists. Most importantly however as well as getting the private laboratories to talk to the MyHR, we will get them to be neutral in terms of secure messaging, so that important data is available live to all important operational nodes in the healthcare system.
No 6.
The ADHA will work closely with the rapidly developing technology sector to integrate smoothly with emerging technologies and products as they arise, especially agile patient app initiatives such as MediTracker and any other mobile patient-centric information ventures where the MyHR can add valuable data not easily accessed by these systems alone. Other systems might include the mobile apps for the major patient management vendors and perhaps the large appointment engines, which are moving to deliver patient-centred services that benefit the whole system.
No 7.
The ADHA will, where it is obvious that private providers can fill a space, not compete with but facilitate the advance of such providers, find the sweet spot of integration, and as a result save us even more money than it is suggested they might in point 8.
“What we have with this comapct is something the recent DoH compacts with the RACGP and the AMA don’t have. Bold but achievable goals that aim for transformative change…”
No 8.
The Department of Health, duly supporting its now rapidly evolving and agile agency, will release full costings of the savings of all of these initiatives so we can be further emboldened by what is possible if we really did get a centralised electronic records system working. By the end of the compact period (nine months) it will be clear that the $305 million in savings from the project which were identified as being realisable over the forward estimates of the recent budget, have well and truly started. And might be even better than predicted.
No 9.
That there will be a rational and effective education, training and awareness campaign of both the public and for healthcare professionals, which will be measurable and stage gated so we can adapt if required. Our measure of the success of the campaign will be with hard metrics that point to tangible changes in the system. We will try hard to make the product market itself, through it’s utility. We will also seek to use GPs as effective marketing hubs for their patients. We know this will only be achievable if we make the product truly attractive to doctors.
No 10.
That by the end of the nine-month period, the MyHR project will have finally shown itself to be the right project for us all to have embarked upon. And that between the savings and the lives improved or saved, there will be largely a positive aura starting to develop around the project. It might even be that the project starts to draw much of the healthcare community together, increasing the potential for further substatnive step change improvements to the delivery of healthcare in Australia.
That is a compact!
And just to be sure, we at The Medical Republic are allocating 10 marks to each point in the compact. And we are going to mark it at three, six and nine months.
Frankly, we think that anything over a 50% mark by month nine,should be seen by even the most hardened cynics of this project as something of a spectacular job by the ADHA, its CEO Tim Kelsey, and the DoH. OK, the project will have burnt nearly $1.5 billion to get there. But if those in the ADHA and DoH can swing this project, as they imply they can, why wouldn’t we try to help them get there?
I’m going to make a long-odds bet on the mark being even higher than 50%. The reason being, we all need to be positive during this period and do all we can to give this thing it a big fat shove.
There are allegedly some idealogues out there who still will say the project has no hope, that it is and always was fundamentally flawed. There is a well known group of what we could term “fundamentalist opt-inners” who say that by going to “opt out” the MyHR is already doomed.
I don’t think so. But that is a complex argument which we won’t examine in this peice.
I think that with enough commitment, energy and smarts, it is just possible to tip this project into something that pays respect to its original vision. The signs to date have been slim that a turnaround is possible. But the new ADHA is still young at only 10 months old.
What we have with this compact is something the recent DoH compacts with the RACGP and the AMA don’t have. Bold but achievable goals that aim for transformative change, hard benchmarking of results, stage gating, a means of monitoring accountability for spending and simplicity.
I don’t think it is going to be easy, or even pretty. It is an extraordinarily hard compact to deliver on given the ADHA legacy and where they are starting from. But if I’m reading things right, they are up for it. They really want to give it a shake. And they are a capable and well re-organised group these days.
The clock starts today. The ADHA has nine months. Actually, they only have a couple of months or less to their first stage gate: the enlistment of the private pathology fraternity – to create enough gravity of data in the MyHR for it to be truly able to tip in the manner described in this compact.
These are exciting times. I hope everyone sees this compact for what it is and gives it all their support and constructive criticism. And we should all endeavour to keep the players honest to their compact initiatives as specified.
If we give it our all, and we don’t play politics, commercial tic tac toe, or my brilliant career games, and it still doesn’t work? We will have at least put this thing properly to bed. So we can move on.
Next Week: A compact between the big private labs, the government and the Australian public (nudge, nudge, wink, wink).
