
Spending more on healthcare has little impact on improving key health outcomes, writes Chris Doucouliagos
A new analysis has found spending more on healthcare has little impact on improving key health outcomes. It found that a 10% increase in health-care spending reduces the number of deaths by only 1.3%, and increases life expectancy by only 0.4%.
Our new meta-analysis, which pooled results from 65 studies, looked at healthcare spending by both the private and public sectors including preventive and curative care.
Healthcare spending as a share of GDP has nearly doubled in OECD countries since 1970. Death rates fell in OECD countries by 86% during this period. While this is a great achievement, given our study found health spending improves death rates by only a small amount, the doubling of spending explains only a small fraction of this large improvement in health. This is because healthcare spending is only one of many factors that affect health.
Our analysis looked at two measures of health: life expectancy and death rates, which are major health status indicators. These are two of the most important measures of health status, but health care treats a large number of diseases and conditions not investigated by our study.
Our analysis also showed public healthcare spending is more effective in reducing death than private spending, contrary to some earlier studies. We found no real difference between the effect of spending on health in developed and developing countries, or between genders.
Wealthier countries spend more on health
Healthcare spending per person has risen throughout the world. In 2014, the high-income OECD countries spent, on average, the equivalent of US$4,698 per person on health. In Australia we spent US$4,357 per person. These amounts are significantly higher than the global average of US$1,276 per person.
Over time, spending on health has been diverging between high-income countries and the rest of the world, with spending in high-income countries growing faster than in other countries. This raises the issue of value for money, especially in the USA where spending is US$9,403 per person. This is despite having pretty poor outcomes compared to money spent.

Even though spending is diverging among countries, some health outcomes are becoming similar over time between developed and developing countries. For example, child mortality has fallen throughout the world but the fall has been greater in non-OECD countries.
In 1960, child mortality in OECD countries was 63 deaths per 1,000, compared to 183 in the world as a whole. This is a difference of 120 deaths. By 2015, mortality in the OECD countries fell to seven deaths per 1,000 and in the world as whole mortality fell to 43.

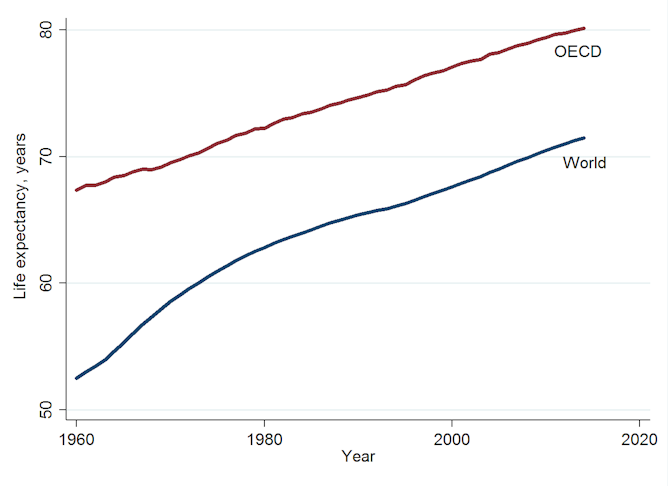
And while life expectancy has increased globally, the gap between OECD countries and all countries has remained largely unchanged.
So where should the money go?
So it follows from our study that household income, education, wealth inequality, demographics and lifestyle choices play a collectively more important role in improving health. Lifestyle choices include nutrition, physical activity, and the consumption of alcohol and tobacco.
Some health-care spending is wasted on unnecessary procedures, slow uptake of generic drugs and administrative inefficiencies. Some of this is possibly due to the influence of powerful interest groups such as the pharmaceutical industry and medical bureaucracies.
The finding that public funding of healthcare results in a slightly larger reduction in premature death than private funding highlights the importance of directing funding to government hospitals and other public health measures. Progress in medical technology – for example, in fighting cancer and heart disease – is especially important and warrants additional funding.
This article was first published on theconversation
Author Chris Doucouliagos is Professor of Economics, Department of Economics, Deakin Business School and Alfred Deakin Institute for Citizenship and Globalisation, Deakin University
