
Owning a GP practice isn’t as bad as the whingers say, but it’s not the winning lottery ticket some people want you to believe it is, either.
I was minding my own business late last week when someone lobbed this letter at my inbox from a passing metaphorical truck, without any accompanying comment, documentation or source.
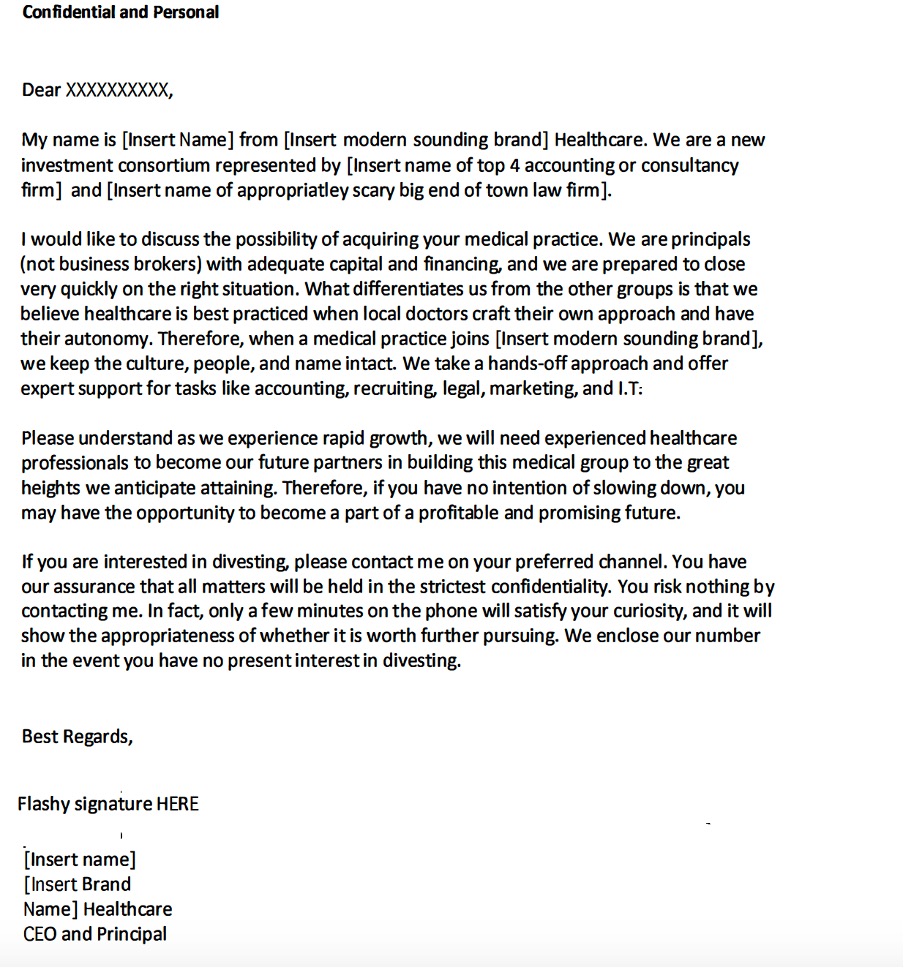
I have taken out names to protect the innocent (or guilty) and inserted notes just in case you’d like to use the template and start your own version of a modern GP dot-com-type runaway success story, and enter the heady world of mergers and acquisitions, scaling businesses, fame and high finance.
Thank you, metaphorical truck driver.
This letter was funny. A bit Nigerian Prince email and cheesy, but funny.
Except that I checked – and it turns out to be a real and apparently serious letter and offer.
Which makes it not quite so funny.
I probably would have realised this earlier but I had failed to read the attached note on the eminent board of this new consortium, complete with potted CV of each board member. The thing is, nearly everyone on the board of this new venture is eminent. It includes an ex and well-known head of a huge healthcare provider, from a famously rich family, a well-known and very smart professor of medicine, and a well-known medical college identity.
When you read who is on the board, you definitely stop and think about whether there might be something these guys know that you don’t. After all, why would all these eminent people be on the board?
The board addendum has the alluring aroma of FOMO about it.
The consortium is connected to some high-end lawyers and accountants (which anyone can be, by hiring them, of course) and apparently has some money with which to buy your practice. It feels like the board of this particular consortium constitutes its major selling point, for anyone who might actually be interested.
If they are in, and backing it (there is nothing saying they are financially backing it, but they are on the board according to this letter, so they are in terms of their reputations and we guess there would be some monetary reward, at least) then they must know something, right, or they wouldn’t be in?
They wouldn’t be risking their reputations, right?
No, they probably wouldn’t be risking their reputations.
Not knowingly.
But beware the eminent person who might be a bit overcommitted from time to time and plays the field of the lots of ideas being pitched at them.
The board members of the failed and fraudulent billion-dollar blood-testing start-up Theranos (whose founder Elizabeth Holmes is on trial as we speak), which included George Shultz and Henry Kissinger, didn’t take part knowing that the technology never worked and probably never would. Nor did the board of Crown understand that it was a cash-laundering business for Asian triads, not a leisure business. They should have known, given their eminence and experience, but they didn’t.
The fact is, a superstar board guarantees you just about nothing these days. It can be something of a red flag, even.
Of course, no one is saying that this outfit is fraudulent or up to mischief. They most likely mean well and want to make everyone lots of money. Who doesn’t?
And at least the board of this venture have some collective experience in general practice and medicine – the board of Theranos seriously lacked the sector experience or they might have smelt something wrong a lot earlier.
But is this a board experienced in building the largest new corporate GP outfit in Australia from nothing, against the might of several major competitors in a global business, such as Sonic, the private-equity firm BGH, our largest private health insurance operator and a few very experienced and wily operators from the past?
Is this a board experienced in mergers and acquisitions, roll-ups, health technology, building a new and large general practice corporate model, running and scaling complex businesses, governance, government policy, building systems, and so on?
Well, they’ve got some of that. But that might be the problem. They have some of the parts, but not the sum of the parts. It’s nearly all optics and no strategy – that you can see anyway.
While there’s probably no doubt that the board has bought into the idea put to them, and they probably think they could contribute meaningfully to that idea, and they mean well (who doesn’t?), it’s not all that likely that they themselves can make this venture successful in any way.
They aren’t going to build the company. They all have other jobs and those jobs aren’t anything like the kind of job needed to build a new GP corporate that could somehow outcompete the established positions, brains and capital behind the likes of BGH, Medicare, Sonic, Healius, Cornerstone, Better Health and an array of other pretty well-run (and growing) and determined corporates out there.
General practice seems to have an interesting future, given its pivotal role in a healthcare system that will need sophisticated and networked chronic care management in the community. But you don’t have to be much of a researcher or a genius to work out that there isn’t anyone out there – smart PE and big money included – who currently has a firm understanding about what that future actually might look like, or how you might build a business around what is evolving today that would be successful in the future.
In fact, so far, mostly the opposite is true.
Building and running a big rollup of GP practices is a bloody hard road to tread at the moment, and likely to be for some time yet.
Yes, there are some smart ones that are making money. But the risks, the complexities, the unknowns around Medicare and government policy, the swings and roundabouts of the current pandemic, the fallout from the pandemic, budget wise, in healthcare that is coming, the decline in GP supply, and structural issues facing the profession, remain very significant issues for such businesses.
Of all the businesses you’d want to run, you wouldn’t want to run a GP corporate. It pretty much has the royal flush of structural and cultural challenges that any business can face: massive culture and technology change that is going to be hard to manage and predict; natural resistance and difficulty in scaling; heavy reliance on government policy; huge governance requirements; supply of the right kind of labour, supply of labour full stop; lack of skilled and experienced management in the sector; transformative technology change, and so on.
Of course, in such difficulty there will probably be opportunity one day. And for those bright individuals who persist, work hard enough, and bring the right combinations of experience, knowledge of the sector, intellectual prowess, technology integration, hard work and, probably to a large degree, commitment to the sector, there probably is some future.
But this letter isn’t offering any of that.
This letter is chum in the water of uncertainty in general practice at present for unsuspecting and tired GP owners who think that maybe, just maybe, there is such a thing as a free lunch finally.
There isn’t.
But do you have anything to lose by calling?
I guess if they want to buy your practice for 10 times its worth without asking too many questions, you might not.
But there’s that free lunch thing again.
One thing you might do before you pick up the phone is Google the name of the company, and maybe check it is even a company by doing a free ASIC look-up. In the case of this particular offer the name of the company doesn’t exist anywhere I can find except on the letter and the LinkedIn profile of the founder writing the letter. No website, no registered business name, no registered business in that name nor another carrying the business name.
That immediately poses the question: Is the board in the letter really a board in the true corporate governance sense?
I myself wouldn’t bother ringing after getting this far.
You’re almost certainly wasting your time if the entity hasn’t even got their act together to constitute an actual company with a proper board, but is advertising to you in your first introduction to them that they have a board. This is a business technique called ‘fake it til you make it’. You don’t want to be early in a business that someone is ‘faking it’. Mostly it only goes downhill from there.
If you are interested in valuing your business in these strange times and possibly offloading it to a corporate or even developing your own roll-up strategy with some friends, a letter like this isn’t the place to start. There are people who advise GP practices for a living and understand a good deal more about what is behind a letter like this than you probably do. If your curiosity is sparked, find one of these people and have a chat. I’m sure the initial chat won’t cost you anything.
As you might already be aware, this consortium and their funny letter aren’t the only game in town pitching for your wares in slightly off-hand ways, unfortunately.
Things are starting to become decidedly nutty out there in GP Owner land at the moment, as far as what your GP practice might now be worth and what you should do should it be worth a bit more now.
It’s all a little “dares gold in dem dar hills”. But in this case, no one has actually struck the gold yet. They have just observed some geography that feels like it could bear gold. And then added a bit of speculative narrative.
You might want to blame one of our best local private equity groups, BGH, for seeding this faux gold rush by deciding to buy what looked like some pretty tired, troubled and ragged corporate GP centre assets from Healius for more than 10 times EBITDA a year or so back.
What did they know?
After all, aren’t they the smartest PE game in town?
PE isn’t going to tell you why they did it.
But you might do well to try to find out why Healius decided, after years of trying to reinvent the business and a lot of investment, to sell it.
Not long after BGH, a few other deals gave BGH’s acquisition some credibility momentum.
Medibank acquired half of Myhealth for a similar price multiple (ironically from a PE firm: why did they sell, you should ask?) which seemed to underline the BGH acquisition decision on the value of these assets, although Medibank were claiming their buy was more strategic.
PE buys specifically to resell not that much into the future, once they’ve fixed something up, or what they bought naturally gets much better as a result of a market cycle.
Strategic buys are strategic for an existing company – bought because of some synergy that might be realised when added to another company. As such, they can sometimes attract a premium depending on what the strategic buyer has in mind in terms of adding value to their existing business and strategy. Which might give Medicare an excuse slightly better than BGH for paying so much.
So, all of sudden the value of a GP practice seems to have shot up, and like property in the Byron Hinterland just before the pandemic, you, your high-end lawyer friend and his accounting mate have come up with the idea of buying up all that land before anyone realises what is happening.
Here are a few problems with you and your friends’ idea:
- Everyone is having the same idea at the same time, so you aren’t actually in front of anyone
- No one has a real clue why the value of GP practices has shot up in the manner that everyone is spruiking – just that because of a few sales in the past year or so, they are somehow worth a whole lot more. This isn’t a good basis for building a new business model. You need a few more well-understood fundamentals and it’s not entirely clear that those who have bought corporate GP assets in the past year or so actually have established those fundamentals.
- Some corporates have been modelling what makes a good roll-up practice target for many years now and have been out there buying or talking to the good targets for a long time. You are even more late to this party than you think.
- Without any fundamentals of why the value is growing, you are in a very typical stock market paradigm. Your main motivation is FOMO, not hard business logic.
- The market has some very savvy and well-capitalised incumbents: what is your plan that makes you think you can outgun these guys? Hint: soporific mission statements such as “What differentiates us from the other groups is that we believe healthcare is best practised when local doctors craft their own approach and have their autonomy” aren’t likely to give you the differentiation you’ll need to get there.
- Sometimes there’s a fine line between an idea and bandwagon. This has a lot more bandwagon than innovative new idea to it.
None of this is to say that general practice, and some forms of business models using the assets and IP of existing practices, doesn’t offer some sort of potential in the right hands, moving forward.
General practice is in a fascinating spot. As hard as running a GP practice is, there is opportunity lurking in the changes afoot.
General practice is the pivot around which the government stands its only good chance of managing the healthcare system far more effectively into the future, albeit this can be bad as well as good for GPs.
Networked chronic-care management in the community to keep people healthier, at home and out of hospitals and aged care homes is the only way the system can move in the long run.
And GPs, in some way, are going to be at the centre of all this.
New models of care are coming, largely based on digital technologies, but surely needing a good set of GPs with the right attitude at the centre managing the ship. No doubt, some smart people are going to leverage these technologies against existing general practice models and assets with a view to inserting themselves with the right model at the right place in the right time.
With $17 billion on the table to sort out aged care, with a cashed-up but in-trouble private health insurance sector that has to reinvent itself more into the healthcare cycle, with rebated telehealth probably here forever, and a range of ground-breaking, new web-based information technologies on the rise, things are likely going to eventually give somewhere.
So do keep your ear to the ground and stay interested in good ideas and people.
Or even better, start something new and interesting that taps into the emerging trends of hospital in the home, virtual care, aged care in the home, and so on.
It is exciting in so many ways.
But none of it is ever going to be easy.
Don’t believe anyone who tells you it is.
There’s never been a free lunch in general practice, and there probably never will be.
