

Shocking mortality from COVID-19 in US care homes, Belgium shows highest population mortality rates, and morbid obesity linked to five-fold higher mortality in younger patients
Thanks for joining us on The Medical Republic‘s live COVID-19 blog.
Thanks to our sponsor and supporter for funding this project with an independent grant, Boehringer Ingelheim.
The latest
- Afternoon update: Shocking mortality in US care homes, Belgium shows highest population mortality rates, and morbid obesity linked to five-fold higher mortality in younger patients.
- Morning update: Cruise ship points to high rates of asymptomatic infection rates; and the latest TMR podcast drops.
- Today’s updated COVID-19 infection figures for Australia
- Some grim figures from data analytics site Statista today on the mortality rates for COVID-19 in US aged care facilities, and COVID-19 death rates more generally. According to their analysis, a staggering 81% of COVID-19 deaths in the state of Minnesota have occurred in long-term care facilities. And it’s not just Minnesota: in New Hampshire, long-term aged care facilities have accounted for 77% of COVID-19 deaths, and in Massachusetts, it’s 61%.
Meanwhile a second article on Statista laid out the COVID-19 death rates per 100,000 population around the world, and Belgium earned the dubious crown of number 1 on the leaderboard with just over 81 deaths from COVID-19 per 100,000. A fair way behind in second place is Spain with 57 per 100,000, the UK at 55, Italy at 54, and way down in ninth place is the United States with just over 30 deaths per 100,000. Just imagine Donald Trump’s disappointment. - Smoking does appear to be associated with more severe COVID-19 and death, according to a review by the World Health Organization.
While there are currently no peer-reviewed studies of the risk of SARS-CoV-2 infection or the risk of hospitalisation with COVID-19 among smokers, the review did report on a meta-analysis of seven studies which found a statistically significant association between smoking and COVID-19 severity. The review also identified several other studies that linked smoking both more severe disease, increased risk of ICU admission and increased mortality from COVID-19. However the association wasn’t clear cut, with some studies finding no significant associations between smoking and COVID-19 outcomes.
“Collecting smoking history is challenging in emergency contexts and severity of disease is often not clearly defined and is inconsistent across studies,” the authors wrote. - A BMI above 40 is associated with a five-fold greater odds of mortality in COVID-19 infection, and the impact of morbid obesity on mortality was greater among younger patients, according to a study of 3406 patients hospitalised in New York.
The study, published in Obesity, found that among patients aged under 50 years, those with morbid obesity were five times more likely to die than those with a BMI under 40. Among the older patients, morbid obesity was also independently associated with an increased risk of death, but a far smaller increase than was seen in younger patients.

- How many COVID-19-infected individuals are asymptomatic? Two more studies published today have grappled with this complex question; one from a cruise ship in which the entirety of its passenger and crew were tested, and one from the testing of contacts of known cases in Wuhan.
The cruise ship study, published in Thorax, tested 217 passenger and crew as they boarded for an Antarctic cruise that went ahead in mid-March despite the pandemic having already been called by the WHO. The first febrile passenger was reported on day eight of the cruise, at which point one can only imagine the ‘oh shit’ sentiments going through the minds of all on board what was to become a sardine-can of COVID-19.
By the end of the adventure, 59% of the cast of this calamity tested positive for SARS-CoV-2 and a staggering 81% of these showed no symptoms of infection. Eight of those infected required medical evacuation, four were intubated and ventilated, and one died.
The authors also noted that despite all passengers being confined to cabins after the outbreak began, there was likely still some illicit cabin-hopping going, because there was evidence of ‘cross-contamination’.
Meanwhile in Wuhan, 78 individuals from 28 cluster cases were tested for SARS-CoV-2 because they had either been exposed to a known contact or visited the Hunan seafood market. This case series, published in JAMA Network Open, found that 42.3% of those who tested positive were asymptomatic, and these patients tender to be younger, more likely to be female, and they also showed shorter duration of viral shedding (recorded using nasopharynx swabs). - Let your ears do the walking … or something like that … and listen to The Medical Republic’s latest podcast, featuring TMR reporters Felicity Nelson and Francine Crimmins, and live COVID-19 blogger Bianca Nogrady, to catch up on all the latest pandemic stories from the last week.
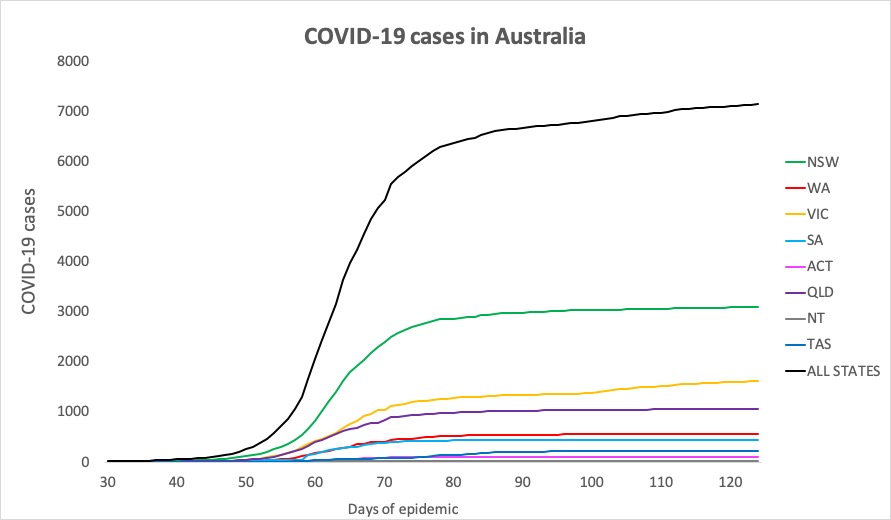
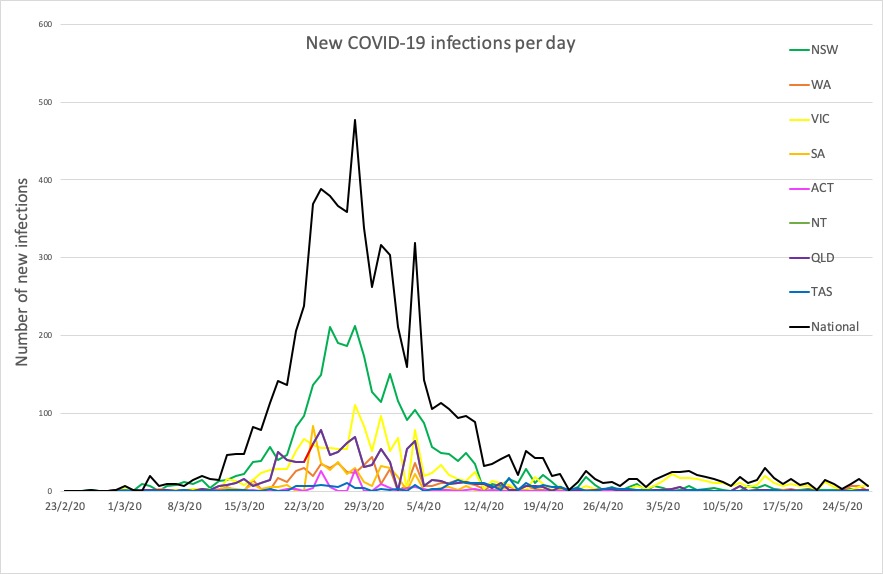
- Here are today’s confirmed COVID-19 infection rates, to 9pm yesterday. New South Wales’ total actually went down by three cases, because five cases were excluded overnight – for unspecified reasons, but possibly false positive results – but the two Sydney students were added to the total.
Victoria recorded eight new cases: three through community testing, one in a returned traveller, two staff members at Lynden Aged Care in Camberwell – which recently had its first case in a patient – and a staff member at a Rydges hotel.
National – 7139, with 103 deaths and 6566 recovered
ACT – 107
NSW – 3089
NT – 29
QLD – 1058
SA – 440
TAS – 228
VIC – 1618
WA – 570
Disclaimer: The content on the Medical Republic COVID-19 blog is independently created by Medical Republic without input from Boehringer Ingelheim Pty Ltd. The views, information, or opinions expressed on the Medical Republic COVID-19 blog are Medical Republic’s own and do not necessarily represent those of Boehringer Ingelheim Pty Ltd. Boehringer Ingelheim Pty Ltd is not responsible for and does not verify the accuracy of any content on the Medical Republic COVID-19 blog.
