

Corticosteroids do not appear to have any benefit in management of COVID-19, according to a non-peer-reviewed paper published on preprint server MedRxiv
That’s it for today on The Medical Republic‘s live COVID-19 blog.
Thanks to our sponsor and supporter for funding this project with an independent grant, Boehringer Ingelheim.
The latest
- No evidence of a benefit from corticosteroids in COVID-19.
- Could D-dimer levels predict COVID-19 prognosis?
- Nearly half of COVID-19-infected residents in US nursing facility were asymptomatic when tested.
- D-dimer levels in COVID-19 patients could be a marker of disease severity and an indicator of mortality risk, according to new data.
In a non-peer-reviewed paper published on the preprint server MedRxiv, researchers reported the outcomes of a retrospective study in 223 patients with COVID-19 – 125 of whom were described as ‘non-severe’ and 98 classified as ‘severe’.
The analysis found that patients with severe disease had significantly higher levels of D-dimer, C-reactive protein, lactate dehydrogenase and procalcitonin on admission. D-dimer also continued to rise during hospitalisation, which the authors said suggested it was most likely related to disease severity.
When they divided the severely affected patients into those who recovered and those who died, they noticed that among those who died, their D-dimer levels kept increasing, while in the recovered group, D-dimer levels dropped 10 days after admission. The levels were significantly different between the two groups.
The authors commented that when they looked at whether prophylactic antithrombotic therapy had any effect, they saw it had improved outcomes in some patients, although they didn’t provide more details on this.
- Corticosteroids do not appear to have any benefit in management of COVID-19, according to a non-peer-reviewed paper published on preprint server MedRxiv.
In a retrospective cohort study, researchers looked at corticosteroid use in 115 consecutive adult patients admitted to a single hospital in Hubei, China, 73 of whom were treated with intravenous methylprednisolone.
The decision to administer corticosteroids was at the treating physician’s discretion, and the analysis found that those in the corticosteroid group had more comorbidities and lower lymphocyte count.
Nearly one-third of those in the corticosteroid group had adverse outcomes – death or admission to intensive care – compared to 11% in the non-corticosteroid group. After adjusting for disease severity, the researchers still found a higher risk of adverse outcomes with corticosteroids although this was not statistically significant.
Acknowledging it was a small sample size, the authors said their results did not suggest any benefit from corticosteroids.
“Considering the severe complications triggered by glucocorticosteroid such as psychosis, viraemia, diabetes and avascular necrosis, the patients might be more likely to be harmed with such treatment,” they wrote.
- A COVID-19 outbreak in a nursing facility in the US infected nearly two-thirds of residents but nearly half of those infected were asymptomatic at the time of testing.
In a paper published in the New England Journal of Medicine, researchers reported on an outbreak which began with one case and spread to 57 of the 89 residents. After the initial case, researchers screened 76 of the residents twice – one week apart – for COVID-19, regardless of whether they were symptomatic or not.
Within 23 days of the first positive test result, 64% of residents were infected. However 27 of those tested were asymptomatic when first tested, and 24 subsequently developed symptoms within a median of four days. The most common symptoms were fever, cough and malaise.
Overall 11 residents were hospitalised – three in intensive care – and 15 died, representing a 26% mortality rate.
“Transmission from asymptomatic residents infected with SARS-CoV-2 most likely contributed to the rapid and extensive spread of infection to other residents and staff,” the authors wrote. “Symptom-based infection-control strategies were not sufficient to prevent transmission after the introduction of SARS-CoV-2 into this skilled nursing facility.”
- The other hot debate happening in Australia is about whether schools should reopen.
Approaches vary from state to state; NSW is bringing students back one day a week from May 11 with online teaching to continue the other four days of the week, Victoria is encouraging home-schooling for all students, Queensland is keeping students – except children of essential workers or those who are vulnerable at home – in home-schooling at least until 22 May, but South Australia is reopening schools, preschools and early childhood facilities.
Meanwhile the National Centre for Immunisation Research and Surveillance released a report on 18 cases of COVID-19 – nine students and nine staff – from 15 schools in NSW which found that despite having close contact with 735 students and 128 staff, there were only two secondary cases that were likely connected to the index cases.
“SARS-CoV-2 transmission in children in schools appears considerably less than seen for other respiratory viruses, such as influenza,” the report authors wrote. “This is consistent with data from international studies showing low rates of disease in children and suggesting limited spread among children and from children to adults.”
- There’s heated debate in public, private and on social media about the federal government’s COVID-19 contact tracing app COVIDSafe.
The AMA has come out in support of the app, with AMA President Dr Tony Bartone saying he’ll be downloading the app and encouraging others to do the same.
“Contact tracing is currently a slow and labour-intensive process that is essential to slowing the spread of the virus,” Dr Bartone said in a statement. “Speeding up contact tracing to slow the virus spreading will prevent illness and allow an earlier lifting of social distancing and other measures.”
The Australian College of Rural and Remote Medicine also backed the contact tracing app, arguing the benefits outweighed the perceived risks, and that it was a positive step.
ACRRM President Dr Ewen McPhee said he had been “quite dogged” in seeking information about possible privacy and security issues with the app, and that the information storied was only accessible if a person was diagnosed with COVID-19 to enable contact tracing of anyone in close proximity to that person.
There are some concerns that the app might not work as well on iPhones, because the Bluetooth functionality could be reduced when the phone is in low power mode or if it’s competing with other Bluetooth functions.
On Twitter, journalist Mike Carlton sought opinions from healthcare professionals, and received a range of responses:
Question. ONLY for epidemiologists, pathologists, paramedics, ICU nurses, doctors and surgeons.
Would it help you if Australians downloaded this new COVID-19 app ?
— Mike Carlton (@MikeCarlton01) April 26, 2020
Meanwhile Nobel Laureate and immunologist Professor Peter Doherty said he would be installing it:
#Insiders I’ll be signing up for the COVID-19 App. Anything that helps us wrestle COVID-19 to the ground is a plus. Any privacy any of us had pretty much disappeared when we started using mobile phones, searching on line, buying stuff from Amazon or whatever.
— Prof. Peter Doherty (@ProfPCDoherty) April 25, 2020
What do you think? The Medical Republic wants to hear from you about your plans regarding the COVIDSafe app:
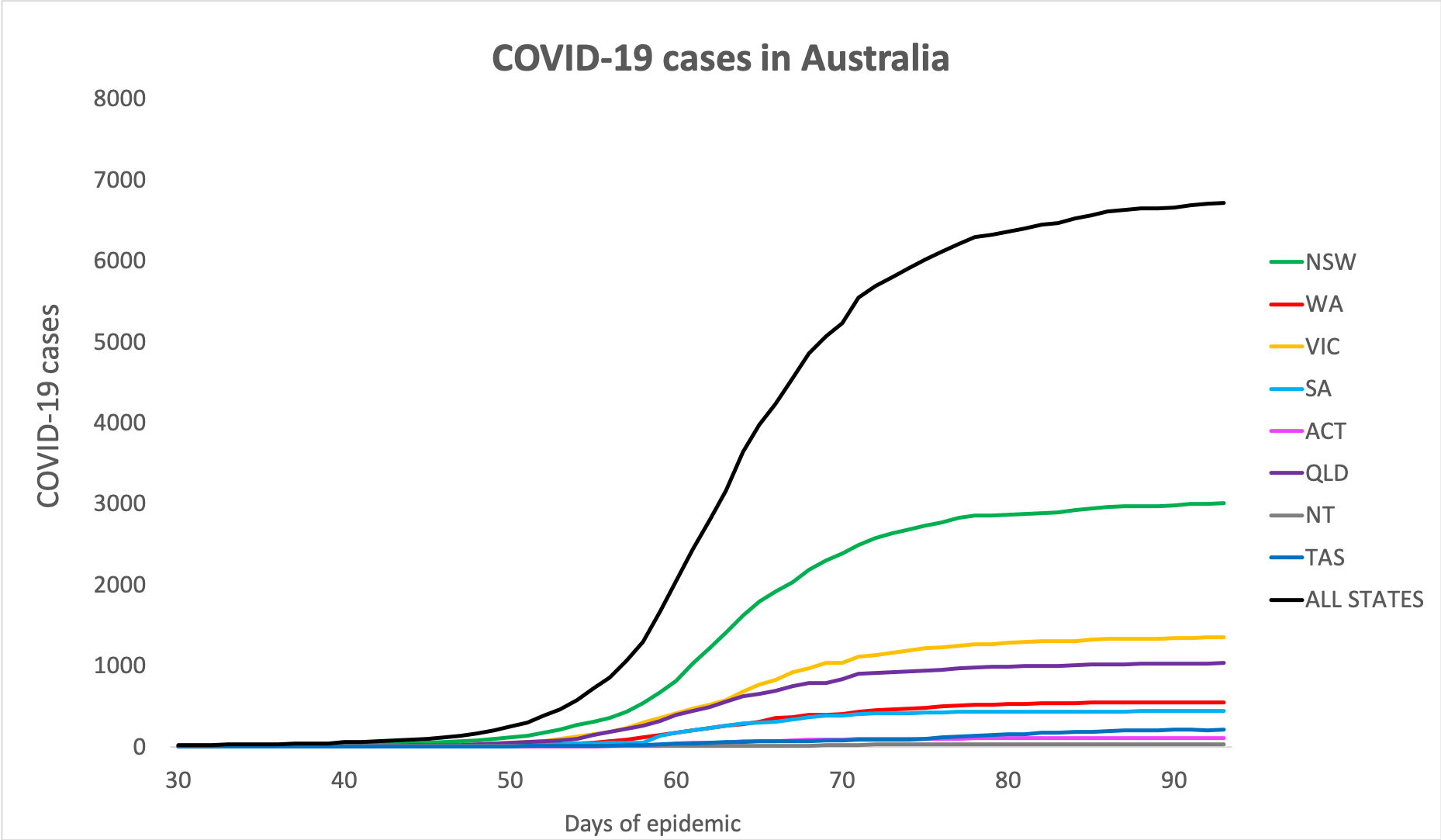
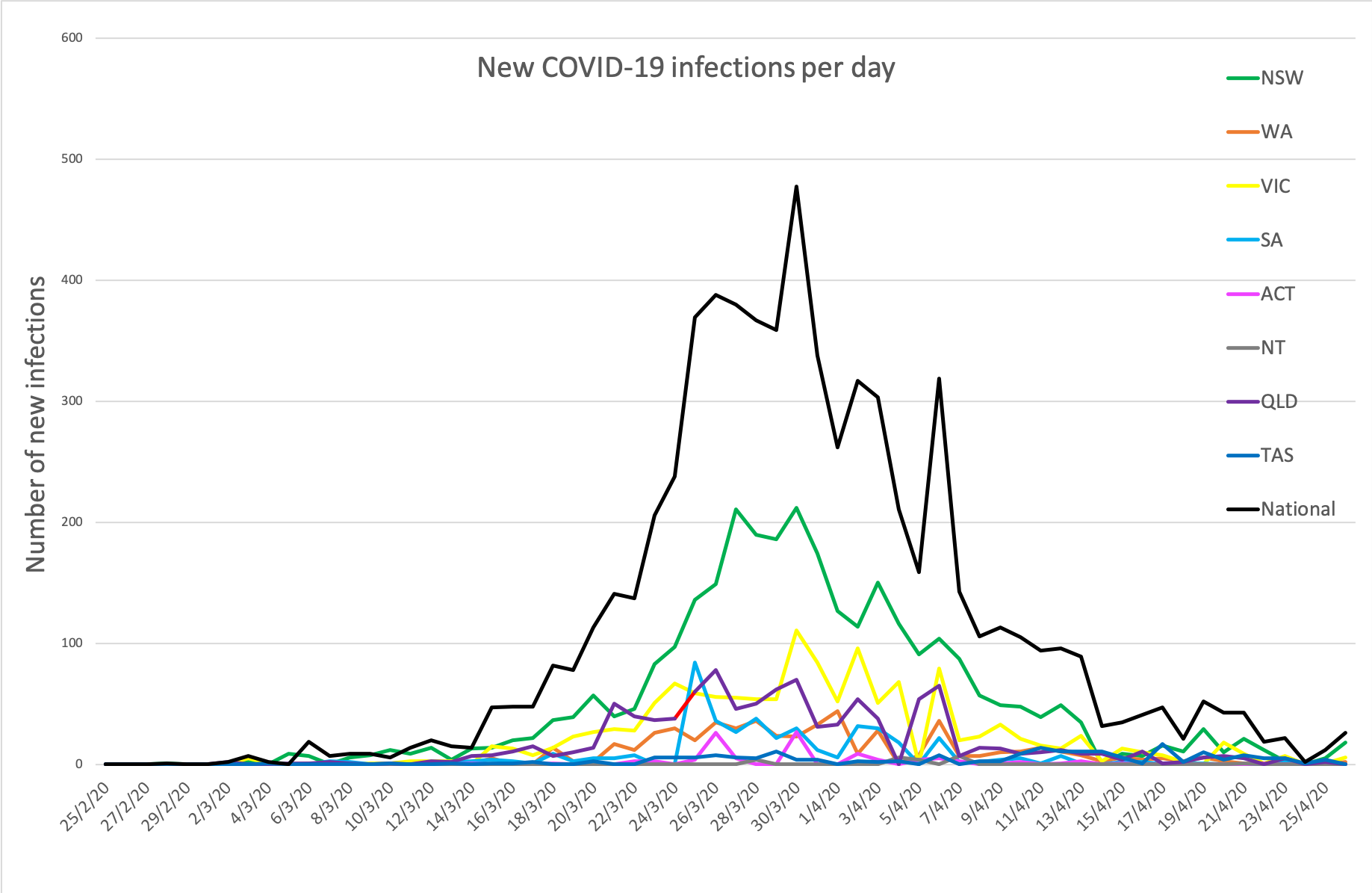
- The overall infection figures are looking flat enough to balance a plate on (see graphs below), but there has been a slight surge in new infections over the weekend, mostly in NSW. Here are the figures to 6am this morning:
National – 6713 (up 10 since yesterday), 83 deaths and 5558 recovered.
ACT – 106
NSW – 3004
NT – 27
QLD – 1030
SA – 438
TAS – 210
VIC – 1349
WA – 549
Disclaimer: The content on the Medical Republic COVID-19 blog is independently created by Medical Republic without input from Boehringer Ingelheim Pty Ltd. The views, information, or opinions expressed on the Medical Republic COVID-19 blog are Medical Republic’s own and do not necessarily represent those of Boehringer Ingelheim Pty Ltd. Boehringer Ingelheim Pty Ltd is not responsible for and does not verify the accuracy of any content on the Medical Republic COVID-19 blog.
