

No one with any symptoms of acute respiratory infection or who has had any contact with COVID-19 cases or travelled in the previous two weeks should enter an aged care facility, says the Australian Health Protection Principal Committee
That’s for a relatively quiet day at The Medical Republic‘s COVID-19 live blog.
Thanks to our sponsor and supporter for funding this project with an independent grant, Boehringer Ingelheim.
The latest
- Residential aged care advice for reducing risk of COVID-19.
- Updated US guidelines recommend against hydroxychloroquine or lopinavir/ritonavir except in clinical trials.
- Clarification from AHPRA about professional indemnity insurance during COVID-19 downturns.
4.04pm, 22 April
If you didn’t get time to read this live blog over the past week but you’d like to hear the latest updates for GPs, we’ve got you covered! In this podcast episode, we provide a summary of what’s been happening:
- As Australia sails nervously into influenza season with COVID-19 hanging from the mast shouting out misdirections, spare a thought for UK GPs heading into hayfever season. The Royal College for General Practitioners has issued advice on how to distinguish between hayfever and COVID-19, which can share common features of stuffy nose, sneezing, eye problems and sometimes cough.
Professor Martin Marshall, Chair of the Royal College of GPs, pointed out that allergy symptoms will generally be milder and fluctuate over the course of the day as pollen levels change. They may also be less severe during wet weather.
“In instances where a patient experiences a significant deviation from this, or have specific symptoms of COVID-19 – a new, persistent cough and a high temperature – we urge them to follow government advice and self- isolate,” he said in a statement.
- As COVID-19 outbreaks in Australian residential aged care facilities claim more lives, the Australian Health Protection Principal Committee has recommended that no one with any symptoms of acute respiratory infection or who has had any contact with COVID-19 cases or travelled in the previous two weeks should enter a facility.
They advised that residents being admitted or re-admitted from other health facilities should be screened for COVID-19 symptoms, and should not be admitted if they have any symptoms. All external excursions should be cancelled, and this also applies to large group visits or gatherings in the facilities. Sorry, but no more bingo nights.
The guidelines suggested visits should be kept short and limited to no more than two visitors at a time per day, whether that be family and friends or professional services. These visits should be restricted to the resident’s room, outdoors, or in a specific location set up for visits, rather than in a communal area.
- The US National Institutes of Health has released an update to its ‘living guidelines’ on COVID-19, which expressly recommend against the use of hydroxychloroquine plus azithromycin, and lopinavir/ritonavir or other HIV protease inhibitors, except in clinical trials.
The guidelines from the multi-organisation COVID-19 Treatment Guidelines Panel (which Donald Trump was presumably not a member of) note that there is insufficient data for them to recommend for or against any antiviral or immunomodulatory therapies – or empiric broad-spectrum antimicrobial therapy in the absence of other indications – in patients with severe COVID-19 disease.
They also recommended against the routine use of systemic corticosteroids in mechanically-ventilated patients without acute respiratory distress syndrome, and said there was insufficient data to recommend their use even in patients with ARDS.
While patients who are already taking ACE inhibitors or ARBs should continue with those medications, the panel recommended against the use of those for treatment of COVID-19 outside a clinical trial setting.
- Wondering what you should be doing about your professional indemnity insurance if COVID-19 has forced you to take a break from work? In a new FAQ, the Australian Health Practitioner Regulation Agency (AHPRA) clarifies that practitioners must have appropriate professional indemnity insurance, but if not practising, you can choose run-off cover instead of full cover while your practice is shut down. Appropriate run-off cover will ensure that you’re covered for matters that might arise from your previous practice, says AHPRA.
If your practice has changed significantly – as in you might be seeing fewer patients, or be operating in a non-clinical role – AHPRA suggests contacting your insurance provider to discuss possibly amending your cover.
But they remind practitioners to review their level of cover when they return to normal practice, to make sure they meet the registration standard.
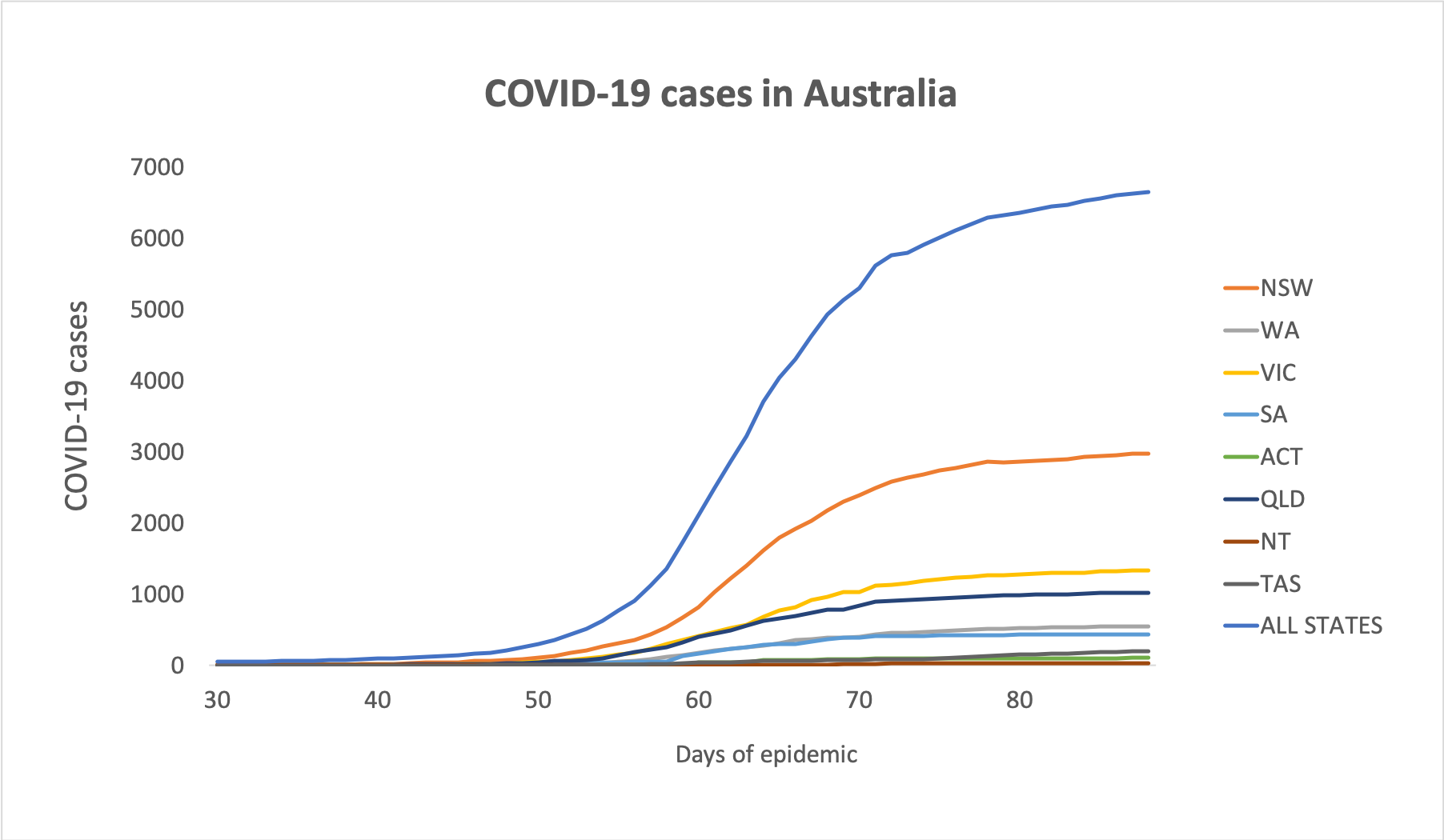
- Here are the latest confirmed COVID-19 infection figures for Australia, to 3pm yesterday:
National – 6,647 (up 22) and 74 deaths
ACT – 104
NSW – 2971
NT – 27
QLD – 1024
SA – 437
TAS – 202
VIC – 1336
WA – 546
- Here are some stories you may have missed yesterday:
New telehealth MBS item numbers for practice nurses and Aboriginal and Torres Strait Islander health practitioners are now available, to enable at-home care for people with chronic conditions, and the government has introduced two new bulk-billing incentives for patients at risk of COVID-19. A study finds physical distancing is based on assumptions of droplet spread from the 1930s, but the evidence suggests respiratory droplets could carry well beyond two metres. Elective surgery will resume from next week thanks to delivery of masks and personal protective equipment, government says.
Disclaimer: The content on the Medical Republic COVID-19 blog is independently created by Medical Republic without input from Boehringer Ingelheim Pty Ltd. The views, information, or opinions expressed on the Medical Republic COVID-19 blog are Medical Republic’s own and do not necessarily represent those of Boehringer Ingelheim Pty Ltd. Boehringer Ingelheim Pty Ltd is not responsible for and does not verify the accuracy of any content on the Medical Republic COVID-19 blog.
