This 79-year-old female presented with bilateral thigh pain of spontaneous onset following long-term bisphosphonate therapy for her osteoporosis.
This 79-year-old female presented with bilateral thigh pain of spontaneous onset following long-term bisphosphonate therapy for her osteoporosis.
There was no history of antecedent traumatic event, recent increase in weightbearing activity, or specific trigger. However, the patient did complain of pain in the thighs on weightbearing. The patient was constitutionally well.
The patient initially underwent radiographs, which demonstrated sclerotic cortical thickening of her lateral proximal femoral shafts, which is a classic appearance for atypical femoral fractures (AFF) associated with bisphosphonate therapy.
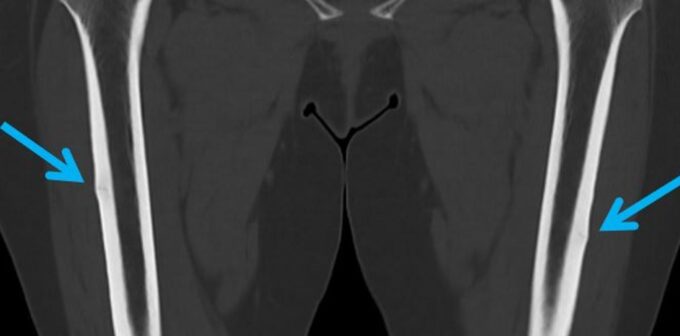
On the subsequent CT, there were lucent linear transverse fracture lines of the lateral femoral cortex with surrounding sclerosis, confirming the presence of bilateral insufficiency fractures of the femora. These are termed “atypical femoral fractures” because of their location, since most insufficiency fractures or stress injuries to the femora occur at the femoral head or neck.
Atypical femoral fractures with bisphosphonate therapy usually occur with minimal or no trauma and present in the subtrochanteric lateral femur as a transverse fracture. They initially appear on X-rays as a small focus of localised or diffuse periosteal thickening that later becomes a cortical “beak” or bump, and eventually results in a lucent linear fracture line if left to progress. Clinical presentation is that of groin or thigh pain. In about 70% of patients, pain in the thigh or groin may be present for several weeks or months before the atypical femoral fracture occurs. These fractures occur bilaterally in up to 60% of patients.
The incidence of these fractures is relatively low (estimated at an annual rate of 2-3 fractures per 10,000 patient-years) but is associated with long-term (>5 years) bisphosphonate use. The risk of AFF with bisphosphonate therapy must be considered against the far greater incidence of common osteoporotic fractures at all sites, and the proven effectiveness of bisphosphonates in reducing the incidence of such osteoporotic fractures.
Management options range from ceasing bisphosphonate therapy and reduction in weightbearing activity to prophylactic intramedullary nail. Teriparatide, an anabolic agent, has been associated with healing of atypical femoral fracture in some cases.
Figure A: Frontal radiograph demonstrating bilateral subtle cortical “beaking” or thickening in the proximal lateral cortex of both femora (arrows)
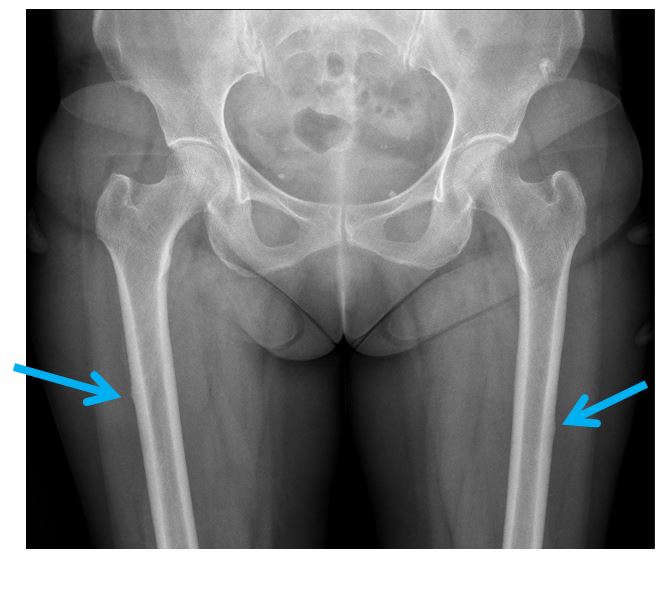
Fig B: CT scan of the same patient confirming bilateral atypical femoral fractures (arrows)
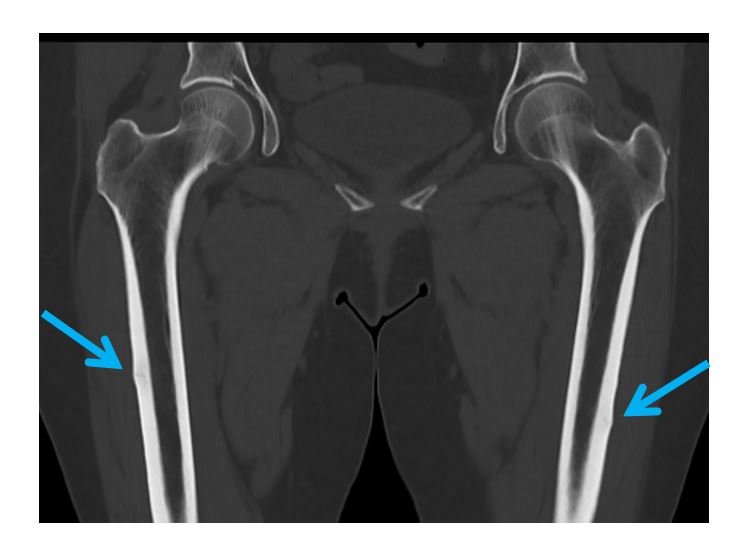
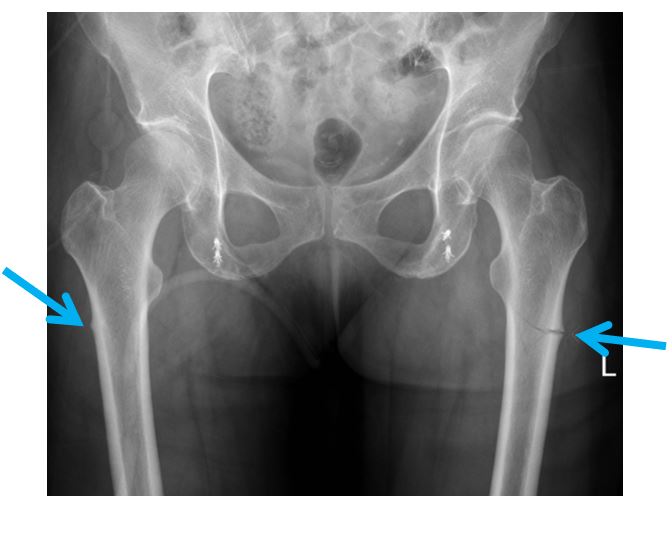
Fig C: Radiographs of another patient – these fractures may progress if untreated


Dr Sebastian Fung is a musculoskeletal radiologist who undertook an MRI imaging fellowship in Hospital for Special Surgery in New York. He now works in Sydney at St Vincent’s Private Hospital and Mater Hospital.
