Australia has very low rates of TB. But the emergence of drug-resistant strains may put total eradication out of reach
It was only three days after Captain Cook’s landing in Botany Bay in 1770 that the scourge of tuberculosis first touched Australia. A seaman who had died from consumption was buried ashore at Sutherland’s Point.
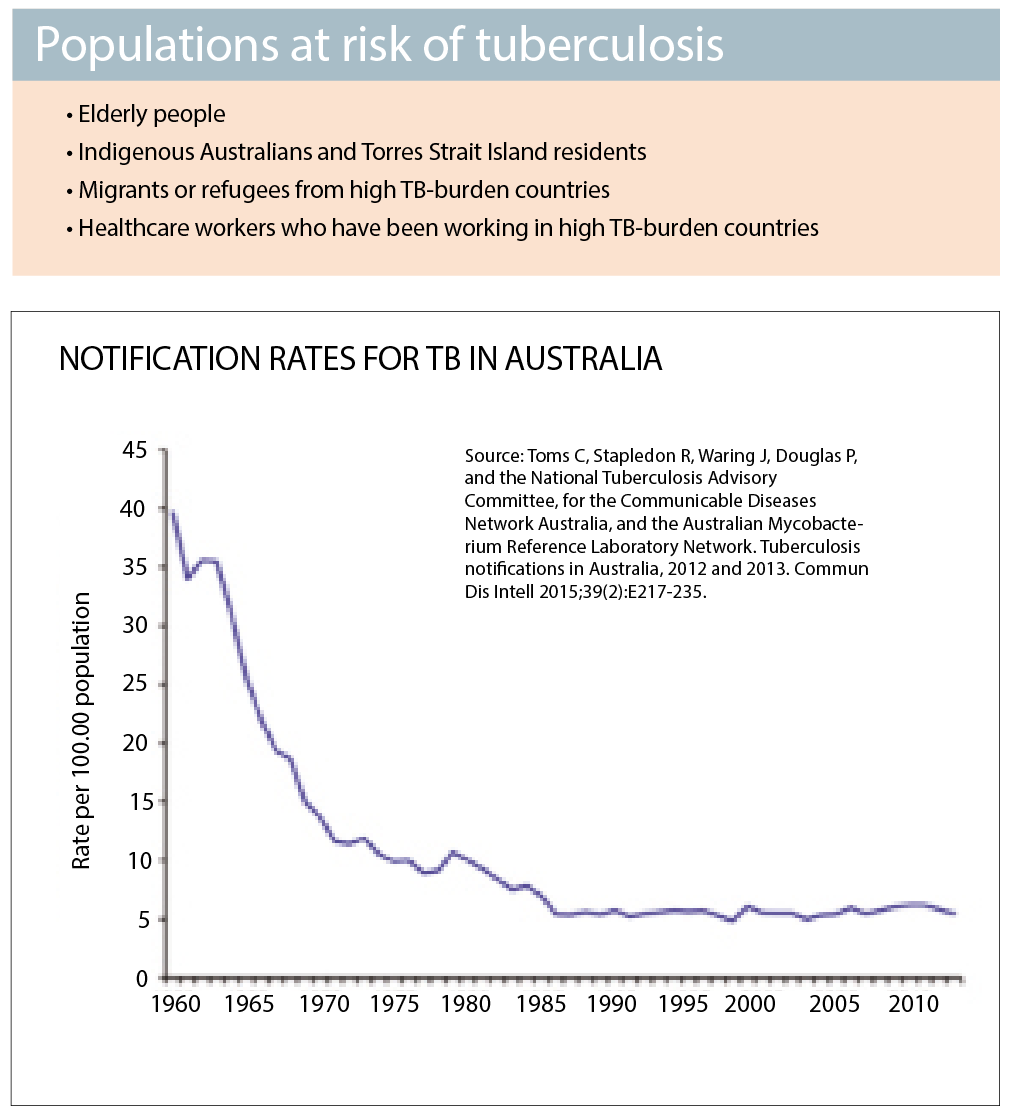
Fortunately, TB is very rare in Australia today. Rates have fallen by 85% since the 1960s and have remained stable since the mid-1980s. Australia now boasts one of the lowest TB rates in the world, with just six cases per 100,000 people. Almost all new cases are diagnosed in people who are believed to have contracted the disease overseas.
The World Health Organisation expects great things from low-burden countries such as Australia. We’re supposed to push TB rates below seven per million by 2035.
That’s almost a 20% decrease in TB incidence rates per year. But experts say we’re not even close to meeting that target.
Globally, we’ve managed to wipe out smallpox and are close to eliminating polio. We’ve practically eradicated measles in Australia. Why is TB proving so difficult?
Diseased planet
TB is now so uncommon in the developed world that it has almost passed out of memory. But just north of the Australian border, our closest neighbour is facing a TB crisis. With around 430 cases of TB per 100,000, Papua New Guinea has a prevalence of the disease that is among one of the highest in the world.
On the small island of Daru, close to the Australian border, more than 160 of the 15,000 population had drug-resistant tuberculosis in 2016. Daru Island General Hospital lacks bed space and specialist wards. It has such poor infection control that at least 13 staff have contracted a drug-resistant strain of the disease.
In Australia, all patients diagnosed with contagious TB are hospitalised for weeks (or months if they have the drug-resistant strain) until they are no longer a threat to public health. Hospital-bed shortages in developing countries such as PNG mean people with active infections remain in the community or return to the community, potentially transferring the infection to others.
Unlike Australia, health authorities in most developing countries have no screening processes in place to actively identify people in the community that may have been infected with TB, says Associate Professor Justin Denholm, an infectious diseases physician and the medical director of the Victorian Tuberculosis Program.
“That’s usually the first thing to fall off,” he says. “People just focus on managing people who are sick rather than trying to prevent cases of disease.”
Despite financial support from the Australian Aid program on Daru, planned population screening and contact tracing cannot be carried out with the resources currently available.
Predictably, TB has begun to spill over the PNG border. The first case appeared on Thursday Island in the Torres Strait over Christmas 2015.
The conditions in which TB thrives in PNG – under-resourced hospitals, poverty, overcrowding and poor nutrition – are also found in many countries. In India, for instance, it is estimated that a patient dies every two minutes from TB.
Countries with a high incidence of HIV in sub-Saharan Africa are particularly vulnerable, as the risk of TB doubles in the first year after HIV infection. Biosocial risk factors commonly present in low-income countries, such as high rates of smoking, diabetes, and pollution also increase the likelihood of contracting TB.
The bacterium Mycobacterium tuberculosis stubbornly remains one of the top 10 killers worldwide. Around 10 million people around the globe had active TB in 2015. Six nations make up 60% of the total TB burden, with India in the lead, followed by Indonesia, China, Nigeria, Pakistan and South Africa.
Australia screens all migrants for active TB, but our borders remain porous. A disease raging on our doorstep is unlikely to ever be completely annihilated.
Gruelling treatment
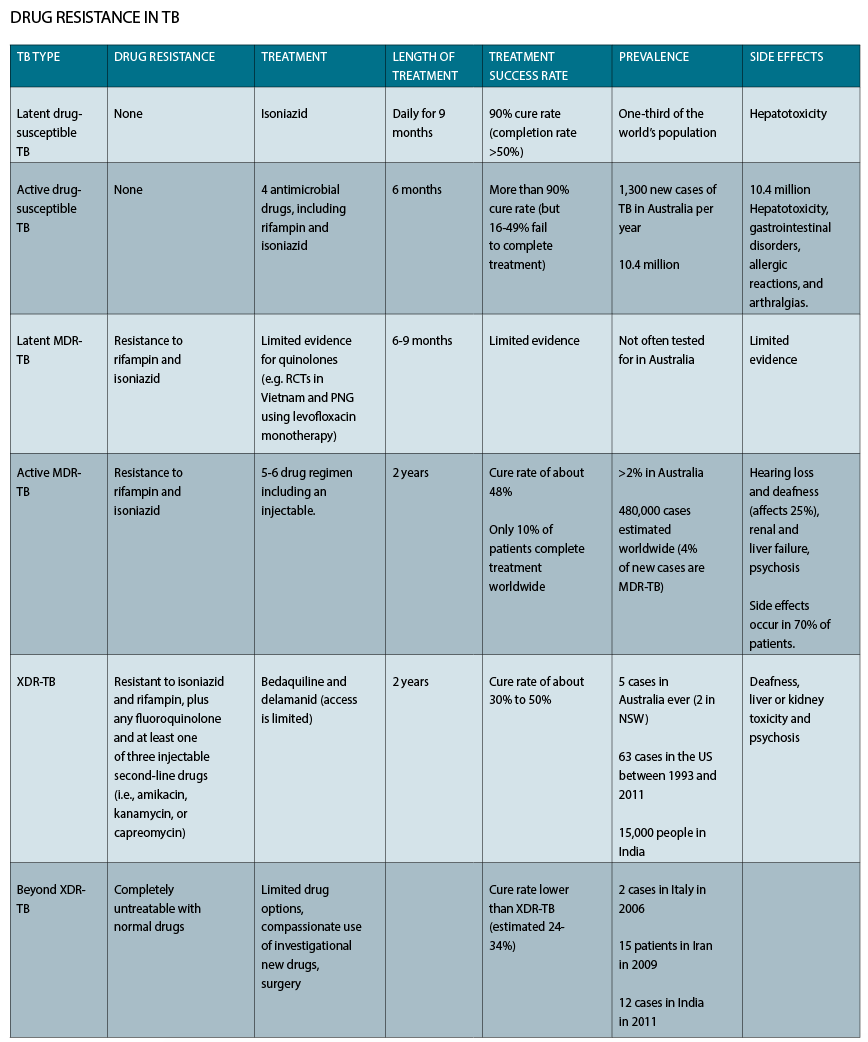
A patient being treated for drug-resistant TB will typically swallow around 13,000 pills and have 240 injection over a two-year period. Even drug-susceptible TB takes six months to cure.
This is an exceptionally long course of treatment compared with other bacterial infectious diseases, which makes ensuring patient adherence, managing side effects and monitoring for toxicity a very challenging task.
Up to 15% of patients experience hepatotoxic effects from TB treatments. And it is estimated between 16% and 49% of patients do not complete the drug regimen.
On top of this, accessing TB treatment can be very time-consuming and expensive. TB patients are required to attend a clinic so that their treatment, including oral antibiotics and injectables, can be supervised.
This system of Directly Observed Treatment Short course (DOTS) was established by the WHO to prevent people skipping treatment and brewing bacterial resistance in the community.
In the Northern Territory, there is a very strict approach to DOTS and all patients get daily observed therapy, says Associate Professor Anna Ralph, an infectious disease physician at Royal Darwin Hospital.
But in the developing world, patients rarely have daily contact with health services, she says. In remote areas of PNG it can take a patient over two hours by bus to reach a clinic, if they even have funds for transport in the first place. The bus fare, combined with the loss of income from missed work, can be “absolutely financially crippling”
How can countries that are not as well resourced as Australia possibly control TB?
“That’s a perfectly fair question, because countries struggle a lot,” says Professor Denholm. “Historically, people have talked about compliance and so forth, suggesting that people fail to complete their therapy. But there is not a lot that patients can do if TB medication goes out of stock at the local pharmacy for weeks or months at a time.
“Those systematic issues … are actually the really critical factors.”
TB time bomb
One of the major reasons TB is so difficult to treat is the rise of antibacterial resistance.
Multidrug-resistant TB (MDR-TB), which is defined by its resistance to rifampin and isoniazid, first appeared in the 1980s. This strain now makes up around 4% of new TB cases and 20% of reactivated cases.
“Because of the amount of drug-resistant TB around the world, it is inevitable that we will get some cases arriving in Australia,” says Professor Denholm. Fortunately, so far MDR-TB is uncommon here, making up only 2% of TB cases over the past decade.
Treatment for MDR-TB is so complex that every case is referred to an expert panel in NSW. This panel includes representatives from Health Protection NSW, the NSW TB program, NSW Mycobacterium Reference Laboratory, the TB co-coordinator responsible for the case, as well as at least three physicians.
“It’s about ensuring the optimal treatment of patients, so that they get the right drug regimen,” says Dr Vicky Sheppeard, Director Communicable Diseases NSW Health.
Of the 67 cases of MDR-TB in NSW over the past 15 years, 87% were successfully treated. A similar hands-on approach is taken in all states and territories.
Patients with MDR-TB are often prescribed 15 or 16 tablets for two years and an injection every day for most of the first year.
One of the “big nasty side effects” of treatment is deafness, which can be permanent, says Professor Ralph. Other adverse effects include loss of balance, nausea and neuropsychiatric reactions.
Sometimes there are so few drug options that patients just have to push through side effects, says Professor Denholm. “There can be some very difficult judgments in that.”
Unsurprisingly, the meticulous management of MDR-TB in Australia is not replicated in poorer nations.
Many countries lack genetic testing technology, such as GeneXpert, to rapidly distinguish between drug susceptible and MDR-TB. The toxicity, expense and length of MDR-TB treatment drags cure rates down to around 10% worldwide.
MDR-TB treatment is often put in the too-hard basket as countries choose to focus on drug-susceptible TB instead of targeting MDR-TB directly.
“Policy makers prefer to treat the problem they can address,” Professor Allen Cheng, an infectious diseases physician at Monash University, wrote in the MJA last year.
But ignoring the problem is creating an even bigger problem. Even scarier TB strains with resistance to the most potent TB drugs, including fluoroquinolone and injectables, started to appear a decade ago.
A total of 63 cases of “extensively drug-resistant TB” (XDR-TB) have been reported in the US, with a cure rate of 30% to 50%. There have been two cases in NSW to date.
In addition to time and medical resources, the cost of treatment rises steeply for drug resistant TB, and few countries can afford the newest medications. Standard TB costs around $62 to treat in PNG, but for MDR-TB the price tag climbs to $12,420. This figure almost doubles again for extremely drug-resistant TB.
And then there’s the fiercest member of the TB family.
In 2006, two women in Italy were diagnosed with what is now called “beyond XDR-TB”.
“This is really winding back the clock to what things were like before we had TB treatments,” Professor Cheng told ABC News. “Some of these strains are completely untreatable with normal drugs.” A further 15 patients infected with beyond XDR-TB were identified in Iran in 2009. Twelve more were reported in India in 2011. Patients with beyond-XDR-TB have been described as “therapeutically destitute”. Their best treatment options are 19th century surgical procedures, such as lung resection, and investigational drugs.
Immigration screening
Another weakness in Australia’s armour against TB infection is its immigration screening program. Around 85% of TB infections occur in people born overseas who acquired TB before moving to Australia.
Immigrants and refugees are screened for active TB with a chest X-ray before entering the country. If TB is detected, they are required to undergo a full course of treatment before travelling to Australia.
Until recently, no immigrants were screened for latent TB, even though people who test positive had a 5% to 10% chance of reactivation within their lifetime. Children under 12 years old are now screened for latent TB, following a change to the policy in 2015.
“I think it would be a very good idea for us to do more testing for latent TB,” says Professor Denholm. “When people are migrating to Australia they are not going to have much risk of being exposed to TB once they come here. So it is a great opportunity for them to start with a clean slate from a health point of view.
“In Victoria, we have an RACGP-accredited training module specifically for the diagnosis and treatment of latent TB. It is a really important way that GPs can be involved in trying to eliminate TB.”
In NSW, there is not a clearly defined role for general practice in latent TB, says Dr Sheppeard. “But this is something that we are starting to examine.”
Testing for latent TB is also important when prescribing immunosuppressants to patients born in high TB burden countries, says Professor Ralph.
GPs can also advise patients that smoking is also a leading risk factor for reactivating TB and try to help them quit, she says.
Uncertainty
Australia would be well on its way to eliminating TB if we could diagnose and cure all TB in the dormant stage. But latent TB is a slippery adversary.
Both tests for latent TB, the interferon-gamma release assay (IGRA) and the tuberculin skin test (TST), are unreliable – producing both false positives and false negatives.
These tests both work by detecting an immune response to TB antigens. Their accuracy can be slightly improved if used in combination with an online calculator, which takes into account where the patient was born, whether they received the BCG vaccine or had direct contact with TB.
Culture of sputum samples can determine whether an active TB infection is drug resistant, and newer molecular tests can give a much faster answer. But there is no test to detect drug resistance in latent TB.
“So it means that we can’t actually tell if someone has been infected with drug-resistant or drug-sensitive disease, unless we know that someone has been exposed from their history,” says Professor Ralph.
Drug-sensitive latent TB can be treated with daily dose of isoniazid for six months. This reduces the risk of children developing TB disease by 50% to 90%. Children up to five years diagnosed with latent TB should be strongly recommended to have treatment and those in the older category should be offered, says Dr Sheppeard.
But the story is more complicated with treatment for latent MDR-TB. There is little evidence to support the various drug regimens, says Professor Ralph. There are a few trials under way using levofloxacin monotherapy for latent MRD-TB in Vietnam and PNG. This drug, which also cures standard latent TB, looks promising, she says.
However, if the toxicity of the drug regimen is too high, it may be preferable to only treat patients who go on to develop an active infection, says Professor Ralph.
“You’ve got to weigh up the risks and benefits,” she says.
Another issue is convincing people to use preventative medication.
“If a child looks perfectly healthy, which they should if they’ve only got latent disease, trying to persuade that family that their child needs a treatment every day for a long period of time is very difficult,” says Professor Ralph.
Vaccine shortage
The BCG vaccine is given to more than 100 million children globally each year. While it does not prevent pulmonary TB, it reduces disseminated disease in children, including TB meningitis and miliary TB.
Since 2015, a global shortage of BCG vaccine due to manufacturing issues has threatened supply, although rapid action to meet shortfalls has minimised infant mortality.
The National Tuberculosis Advisory Committee in Australia found that particularly inconsistent vaccine supply is leading to low, variable and inequitable vaccine delivery. An unregistered alternative product manufactured in Poland is available, but permission must be sought from the TGA prior to use.
The vaccine is indicated for Indigenous children in the NT, who are six times more likely to contract TB than non-Indigenous Australians. Thankfully to date, no increase in disseminated TB has been recorded among NT Indigenous children. The vaccine is also given to children who are travelling to a high TB-burden country for extended periods.
Are we there yet?
Australia is in the envious position of having one of the lowest rates of TB in the world. “If anyone can eliminate TB, Australia can,” says Professor Ralph. To bend the TB incidence curve further downwards, she says, we need to treat latent TB, educate at-risk people about TB, vaccinate infants, and diagnose TB early.
But Professor Denholm says Australia will not meet the WHO targets for eliminating TB with its current approaches.
“That’s not to say that we can’t,” he says. “But for us to do it, we need to greatly scale-up our diagnosis and treatment of latent TB.”
Australia’s national strategic plan to eliminate TB is in its final stages of approval and will be published shortly, Dr Sheppeard tells The Medical Republic.
She wouldn’t give us a hint of what’s in it – but apparently it does align with the WHO goals to reduce TB cases in Australia by 90% by 2030. But there are still many challenges to overcome.
“No one is saying it’s an easy task,” Dr Sheppeard says.