

New lens designs may slow the progression of myopia in children
Myopia was once viewed as a mere optical inconvenience – a refractive error easily corrected with simple, minus-power spectacles. Not anymore.
With rates of short-sightedness hitting an all-time high, optometrists are turning to new lens technologies to try to halt myopia progression.
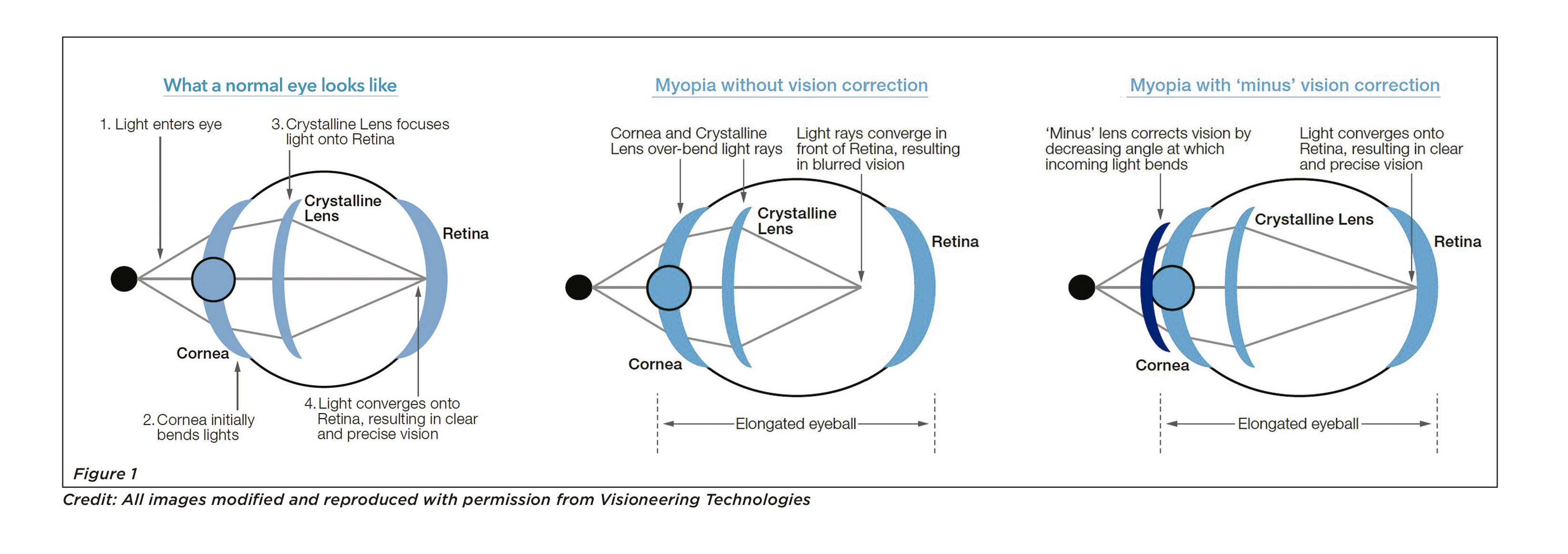
Myopia is an inability to focus on far-away objects caused by elongated eye. It occurs when the cornea and the crystalline lens bend light rays too much relative to the length of the eye.
In people with normal vision, light rays converge precisely on the retina at the back of the eye and form a clear image.
In people with myopia, light rays from far-away objects reach a focal point somewhere in the vitreous humor, which creates a blurry image. (Figure 1).
Myopia usually starts during childhood and gets gradually worse until it settles at the age of around 18-25 years.
Ironically, wearing negative-power spherical glasses to correct myopia may stimulate the eye to grow longer.
By moving the focal point towards the back of the eye for central vision, glasses have the unintended effect of pushing peripheral light ray focal points far beyond the retina.
Some research suggest that the eye grows longer to bring these light rays back into focus, which causes unhealthy stretching of eye tissue – leading to serious eye health problems down the track.
This mechanism has been demonstrated in numerous animal experiments. When plastic minus-powered goggles were strapped over the eyes of newly-hatched chickens, the chickens developed myopia.
Optometrists knew they needed some kind of revolutionary lens technology that could to fix central vision in people with myopia while also dragging the peripheral focal points back inside the retina.
Such a technology really would be a breakthrough because it could, in theory, slow or completely stall the progression of myopia altogether. It would add to our arsenal of atropine and orthokeratology for preventing long-term eye damage from myopia.
Fortunately, there are number of technologies hitting the markets right now that might just do the trick.
(Our podcast episode this week explores myopia in more depth.)
THE BLIGHT OF SHORT-SIGHTEDNESS
Around 30% of the world’s population have myopia. If current trends continue, half of the global population will be myopic by 2050, an estimated five billion people.
“I’m definitely seeing more children with myopia compared with even five years ago and some of them are coming in with quite bad eyesight already,” says Dr Philip Cheng, an optometrist at Eyecare Concepts Optometry in Melbourne.
In the space of just six years, myopia prevalence in Sydney increased from 13% to 30% in children aged 12.
Eyesight is deteriorating at an even faster rate in Asia; in Singapore, 70% of children have myopia; in Guangzhou in China, that number is 50%. Myopia is more than twice as common in UK children now than it was the 1960s, hitting rates of around 16%.
Myopia risk is closely tied to genetics. Having one myopic parent makes you three times as likely to develop myopia. Two myopic parents double those odds.
But genetics alone can’t explain why rates of myopia are climbing around the globe. A range of cultural and technological factors seem to be conspiring to keep children indoors. And kids’ eyes appear to be adapting to life in the near-world by becoming myopic.
“It’s to do with how children use their eyes these days,” says Dr Cheng. “There are a lot more digital devices. It’s also related to education. Kids are spending more time reading, tutoring, learning many different things from a younger age.”
Around 5% of Australian children have severe myopia, which increases their chance of getting serious ocular diseases later in life.
 “Myopia happens when the eye grows physically too long,” says Dr Cheng. “When the eye elongates, it stretches and thins the tissue at the back of the eye – the retina – and it accelerates the ageing process. It’s like a rubber band; if you stretch it too far, it’s going to break.”
“Myopia happens when the eye grows physically too long,” says Dr Cheng. “When the eye elongates, it stretches and thins the tissue at the back of the eye – the retina – and it accelerates the ageing process. It’s like a rubber band; if you stretch it too far, it’s going to break.”
These conditions are normally seen in people aged over 60, but people with myopia can sometimes develop these eye diseases in their 40s or 50s. The risk of macular degeneration increases 10 times for people with middling levels of myopia (between -3 and -6 diopters). For people with high myopia (<-6 diopters), the risk of macular degeneration is 40 times higher. Macular degeneration is very rare in younger people and affects around 3 to 10% of people aged over 55.
Cataracts are common over the age of 65, but myopia increases the risk of developing lens cloudiness at an earlier age. “You might have to have cataract surgery, say, 10 or 15 years earlier than expected,” says Dr Cheng.
Myopia also increases the risk of retinal detachment.
Around half of cases of retinal detachment that aren’t caused by injuries are attributable to myopia in the US.
“It’s fairly rare,” says Dr Cheng. “But you can go blind if you don’t catch it early.”
WHAT CAN BE DONE? In the mid-1990s, Professor Michael Collins, an optometrist at Queensland University of Technology (QUT), struck upon one of the first of many ideas that would help revolutionise contact lenses.
Professor Collins proposed a contact lens that corrected spherical aberration in children with myopia.
Spherical aberration is a slight twisting of light rays as they pass through the lens of the eye. (Figure 3)
In children with myopia, this optical twist moves some of the focal points just in behind the retina, which seems to promote eye growth. By correcting this issue with contact lenses, Professor Collins hoped to block the growth signal and slow myopia development.
He has since filed several US patents for different types of contact lenses for myopia control in partnership with Johnson & Johnson Vision. At this stage, none of these designs have gone to market.
Over the past decade, a plethora of different contact lenses and glasses designs for slowing myopia in children have been patented by various research groups. 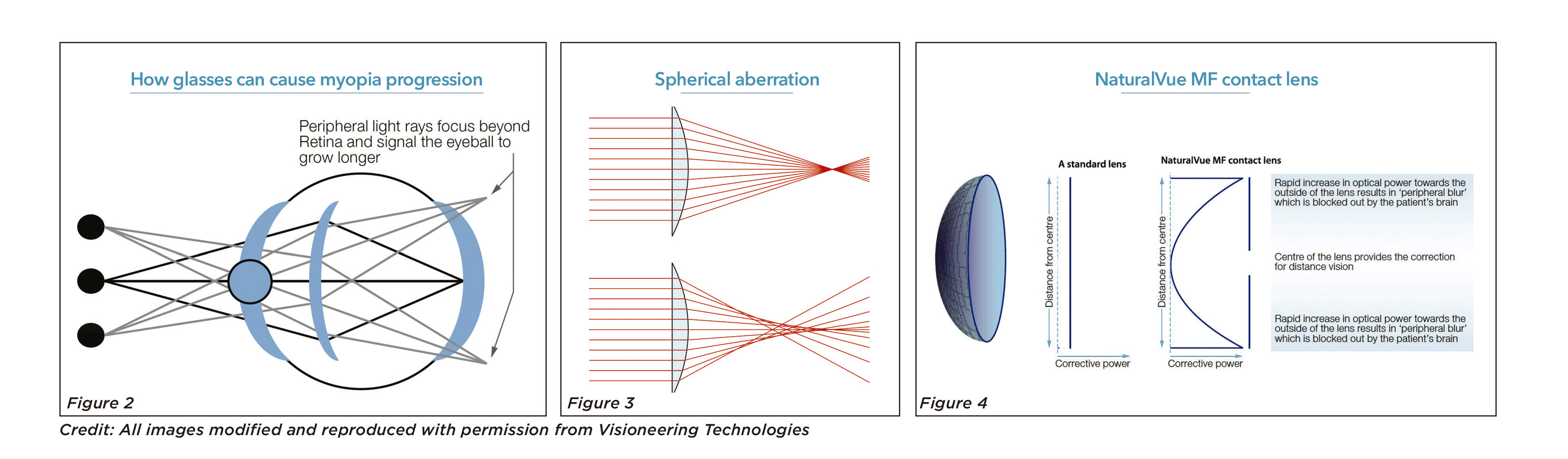
Many of these new technologies are based on a similar concept, says Associate Professor Scott Read, an optometrist and researcher at QUT. Rather than focusing light uniformly throughout, like a standard lens, these new lenses are divided into sections that bring distant light into sharp focus and sections that deliberately blur the light, he says.
How these sections are carved out depends on the design. Some lenses have sudden changes in power from positive regions to negative regions, some have more gradual transitions, and some have multifocal dots scattered across the periphery of the lens.
The Brien Holden Vision Institute in Sydney has patented an extended depth of focus contact (EDOF) lens technology for myopia, which is now distributed by Seed in Japan and McEnnovy in Spain. The EDOF contact lenses slows eye growth by 33-35% when compared to standard single vision lenses.
CooperVision has launched MiSight 1 Day, the first daily disposable myopia control soft contact lenses in 2017. This lens is laid out like a target, with alternating, concentric rings of positive and negative power radiating outwards from the centre.
In a three-year, randomised, controlled study the MiSight contact lens reduced myopia progression by 52%.
Prior to the development of these new contact lenses, orthokeratology was the leading method for slowing myopia progression, along with atropine eye drops.
Orthokeratology involves wearing hard contact lenses overnight to flatten the cornea and correct vision. The lenses are kept for a year or two and must be cleaned every day to avoid infection. Orthokeratology slows the rate of myopia progression by 32-42% over two to five years in children.
There’s a lot of debate around whether low-dose atropine (0.01%) actually slows the progression of myopia in children. Low-dose atropine has minimal side effects and has been favoured as a treatment among ophthalmologists for many years. But more recent research suggests that it may do little to control excessive eye growth.
Another contact lens that was recently TGA-approved in Australia for myopia control was inspired by a very old piece of technology – the pinhole camera.
Humans have known for thousands of years that a tiny pinprick of light in a dark room casts an in-focus, upside-down image on the wall behind. This ancient optical device became known as a “camera obscura” in the 17th century – and was used by early photographers. Pinhole cameras have a near infinite depth of field, which means that everything in the image is in focus.
US optometrist, optical engineer and aerospace engineer Dr Richard Griffin invented a contact lens in the early 2000s that seemed to work the same way.
He created a so-called “virtual pinhole aperture” by placing the patient’s minus prescription for distance at the centre of the contact lens, and then rapidly, smoothly increased the optical power in all directions moving outwards. (Figure 4)
Dr Griffin therorised that everything outside the centre of the lens would appear fuzzy to the patient’s visual processing circuitry, but that the human brain would automatically ignore blurred light, allowing the new contact lens to create a deep depth of focus – just like a pinhole camera.
Like other novel contact lenses, the NaturalVue Multifocal 1 Day aims to push the peripheral light rays back inside the retina and block the growth signals to the eye.
NaturalVue MF reduced myopia progression by around 90% in 141 children aged 12 over six months to four years, according to data presented this year at the Global Specialty Lens Symposium.
Some optometrists in Australia feel comfortable prescribing the contact lens to children based on the available data. They argue that the lens is as good as the alternatives for correcting refractive errors, and there’s no harm from trying it out and seeing if it helps slow myopia progression as well.
Other optometrists have raised concerns about the speed of the roll out. The number of children who have tried the new contact lenses is still small, and these trials were not randomised or controlled, which makes them less convincing.
While the TGA has signed off on the design, some optometrists want to see rigorous scientific research conducted.
GLASSES WITH MICRO-LENSES
At Hong Kong Polytechnic University, a team of researchers have invented a similar product in the form of glasses. The Defocus Incorporated Multiple Segments (DIMS) spectacle lenses slow myopia progression in children by around 60%.
Japanese company Hoya took the product to market in Hong Kong and China last year.
Each pair of DIMS glasses has a central optical zone for correcting refractive error, like most glasses. But the outside of the lens is studded with invisible “micro-lens segments”, which are little dots with positive refractive power.
These micro-lens specks work to bring some of the peripheral light rays back within the eye, thus reducing the signals that stimulate eye growth.
The glasses underwent randomised, controlled, double-blinded testing in 160 Chinese children with myopia between the ages of eight to 13.
The group of children who wore the DIMS glasses had a mean myopic progression of 0.38 diopters over two years, whereas the control group’s progression was 0.93 diopters on average. Around one in five children wearing the DIMS lenses had zero myopia progression, compared with 7.4% of children with single vision lenses.
DIMS aren’t the only spectacles available for myopia control; Essilor has released a pair of glasses called Myopilux.
And Zeiss have a spectacle lens called MyoVision, which also works by inducing peripheral “hyperopic shift”, and delays myopia progression by an average of 30% when compared with traditional glasses.
WHAT OPTOMETRISTS RECOMMEND
The evidence that myopia causes real eye damage over the long-term is mounting up and optometrists are calling for more careful management of the condition.
The International Myopia Institute released seven white papers at the end of last month on myopia progression in children. Around 90 researchers from around the world collaborated on the project.
Dr Kate Gifford, a clinical optometrist based in Brisbane and past president of Optometry Australia, was the lead author on the clinical management guidelines paper.
The papers explain the behavioural or environmental modifications that can help prevent myopia in children, such as outdoor time and taking breaks from near work.
“It talks about contact lens options, spectacle lens options, and pharmacological options,” says Dr Kate Gifford.
“Thus far, the strongest and most consistent research outcomes with least side effects appear to be in the contact lens arena,” says Dr Paul Gifford, a research scientist and industry consultant with a PhD in hyperopic orthokeratology who co-founded the Myopia Profile website with his wife, Dr Kate Gifford. “But there are some kids who are not ready for contact lenses and some that will never be.”
What’s certain is that the traditional method of prescribing single vision glasses is no longer evidence-based, says Dr Kate Gifford.
“That’s not going to do anything to appropriately manage this condition.”
