
Prostatic artery embolisation offers reduced complication rates and faster recovery than transurethral resection, but not enough people know about it.
Benign prostate enlargement or hyperplasia is a highly prevalent condition in Australia, affecting around half of males over 50 and more than 80% of males aged over 80 at some stage in their life.1
BPH can significantly affect quality of life by interfering with daily activities and can lead to complications such as UTIs, kidney damage, and kidney stones.1
Despite the significant health risks, the stigma surrounding certain men’s health conditions, particularly lower urinary tract symptoms (LUTS), can result in a reluctance to seek treatment, increasing their risk of advanced disease states and complications while reducing overall quality of life.2
Current research and feedback indicate that many men are delaying surgical interventions like transurethral resection of the prostate (TURP) due to the fear of side effects and uncertainty about alternative treatment options.3 This can result in years of poor quality of life, disturbed sleep and lifestyle restriction.
Although TURP is the most common and an effective treatment pathway for BPH, it has a high minor complication rate of 64% and a 6.2% rate of severe adverse events.4 The surgery is associated with significant complications, including loss of normal ejaculatory function, post-operative urinary tract infection, post-operative pain, urinary incontinence or retention, haematuria and, rarely, erectile dysfunction. It also comes with increased risks for those with comorbidities and for the elderly, who are at most risk of this condition.
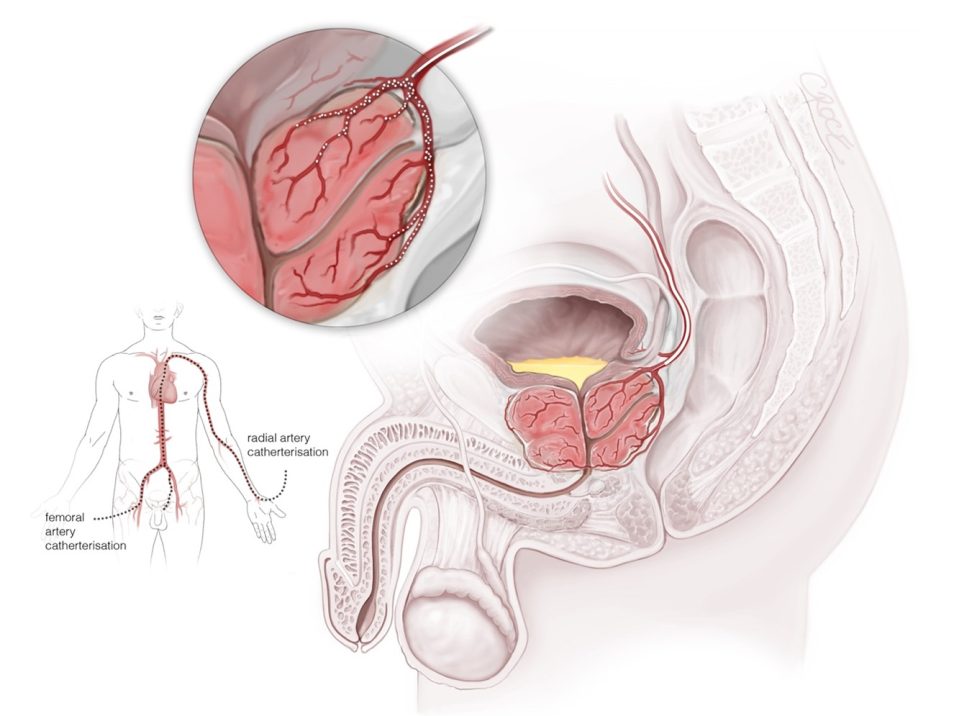
A minimally invasive alternative, prostatic artery embolisation (PAE) has the potential to address these concerns to encourage men to seek timely and effective care for BPH. Performed under local anesthaesia and sedation, it involves reducing blood flow (embolising) the prostatic arteries to reduce prostate size and alleviate symptoms.5 A very fine catheter is inserted into the artery, guided towards the prostate with x-ray imagery.8 Then, the blood flow within the prostate is reduced, which causes the prostate to shrink over time.8 Once that is done, the pinhole access to the artery is sealed with an absorbable plug or compressed. The procedure is generally offered as a day-/half-day-stay process.8

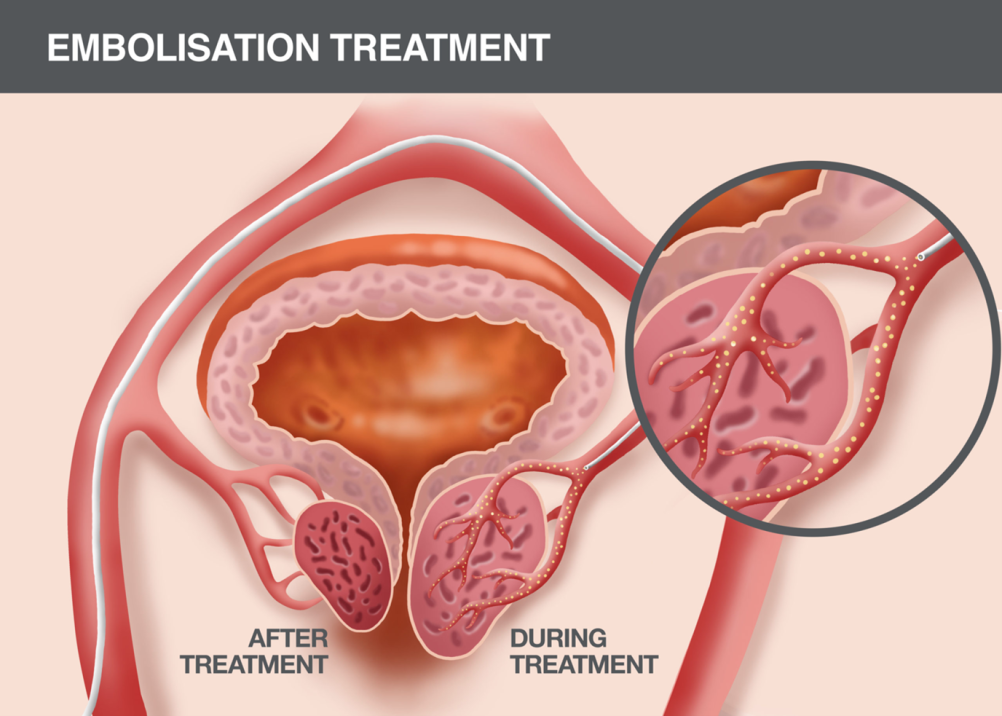
When compared to TURP, PAE offers reduced complication rates and faster recovery5, while delivering similar symptom improvement and quality of life enhancements.4 The associated complications are normally minor and include transient local pain, flare of symptoms and temporary urinary retention. PAE is also associated with fewer instances of retrograde ejaculation and erectile dysfunction, enhancing patient satisfaction.5 Serious adverse effects are rare (vascular complication, serious infection or non-target embolisation).
Since it is a minimally invasive procedure that involves shorter recovery times, PAE is accessible as a lower-cost alternative to surgery.5 While costs will vary doctor to doctor in the private system, it generally has MBS and insurance coverage (embolisation item 35321) which applies in both public and private contexts.
As a procedure that doesn’t require an in-hospital stay, most patients usually return to their daily lives after one day of post-procedure care. Following the average downtime of two days, there is about a 10-day expected period of urinary irritative symptoms (frequency and dysuria) which are treated with anti-inflammatories with predictable improvement after that time.
The American Urological Association guidelines recently included PAE as a treatment option for BPH, recommending that it is performed by interventional radiologists skilled in the technique. Given the many positives of PAE, this comes as no surprise and is a welcome addition after 10 years of accumulated data worldwide and multiple controlled trials. I recently spent time in a leading US clinic, which is a collaboration of interventional radiologists and urologists, and good education and awareness has the clinic successfully performing this therapy for numerous patients daily. In Australia, however, PAE remains an underutilised procedure, mostly, I believe, due to lack of awareness of its existence among the broader community.
The procedure is available at centres around the country, both public and private, in at least a few hospitals in each state. The Interventional Radiology Society of Australasia’s website includes a doctor-finder linking GPs to practitioners in each state who offer the service.
As BPH remains a prevalent condition affecting a large population of Australian men, it’s important to empower these patient groups with information on all treatment options that can meet their health and quality of life requirements. In line with the American Urological Association’s guidelines, it’s time we make greater use of minimally invasive treatments like PAE here in Australia.
Optimising the use of PAE to enhance patient outcomes requires collaborative efforts between specialties.4 While the procedure is performed by an interventional radiologist, our work is only effective as part of a broader multidisciplinary effort from healthcare professionals including urologists and GPs.
My involvement in PAE procedures as an interventional radiologist is preceded by careful consideration with the wider care team to determine whether this is the best treatment option for patients. Thorough patient selection in tandem with holistic pre- and post-procedural consultations are especially crucial for ensuring exceptional patient care.4 GPs play a pivotal role in this process, particularly in the initial assessment and management of LUTS including BPH in men, and in referring appropriate patients to urologists.
Interventional radiologists in Australia (like myself) would be very pleased to consult with patients who are interested whether they are suitable for PAE to undertake a thorough consideration of their circumstances and educate on the outcomes and patient journey for this procedure.6 By exploring PAE as an alternative treatment for eligible patients affected by BPH, healthcare professionals can ensure their patients receive comprehensive and multidisciplinary approaches to their care that can better suit their healthcare needs.7
Dr Chris Rogan is president of the Interventional Radiology Society of Australasia and head of interventional oncology at Chris O’Brien Lifehouse; his interests are in embolisation therapies with application to liver cancer, prostate enlargement and joint conditions like knee arthritis.
References
- Health Direct, n.d. Benign Prostate Hypertrophy. Available at: https://www.healthdirect.gov.au/benign-prostatehypertrophy. [Accessed April 2024]
- Leone, J.E., Rovito, M.J., Mullin, E.M., Mohammed, S.D. and Lee, C.S., 2016. Development and Testing of a Conceptual Model Regarding Men’s Access to Health Care. American Journal of Men’s Health, 11(2), pp.262–274. doi: https://doi.org/10.1177/1557988316671637.
- Emberton M., Marberger M., Rosette J. De. (2008). Understanding patient and physician perceptions of benign prostatic hyperplasia in Europe: The prostate research on behaviour and education (PROBE) survey. International Journal of Clinical Practice, 62(1), 18–26. 10.1111/j.1742-1241.2007.01635.
- Marquis, A., Williams, T. R., McClure, T. D., & Rastinehad, A. R. (2024). The need for PAE – A urologist’s perspective. Endovascular Today, 23(2), 53-57.
- Ini’, C., Vasile, T., Foti, P. V., Timpanaro, C., Castiglione, D. G., Libra, F., Falsaperla, D., Tiralongo, F., Giurazza, F., Mosconi, C., David, E., Palmucci, S., Lavalle, S., Venturini, M., & Basile, A. (2024). Prostate artery embolization as minimally invasive treatment for benign prostatic hyperplasia: An updated systematic review. Journal of Clinical Medicine, 13(9), 2530. https://doi.org/10.3390/jcm13092530
- Yu, H., Isaacson, A. J., & Burke, C. T. (2016). Review of current literature for prostatic artery embolization. Seminars in Interventional Radiology, 33(3), 231-235. https://doi.org/10.1055/s-0036-1586141
- Interventional Radiology Society of Australasia, n.d. Available at: https://irsa.com.au/ [Accessed June 2024]
- Interventional Radiology Society of Australasia, n.d. Prostate artery embolisation (PAE), Available at: https://irsa.com.au/treatments/prostate-artery-embolisation-pae/ [Accessed June 2024]
