
Soft tissue calcification appears in a number of conditions, some of which are quite aggressive.
A 66-year-old female presented with an uncomfortable lump on the lateral aspect of the proximal hip, in a trochanteric location.
This lump gradually increased in size over 7-8 years and was causing increasing pain and tenderness. There was pain on movement, climbing stairs and lifting the leg. There was no history of injury to this region.
On examination, there was palpable, mildly tender hard solitary 4cm lump with no transillumination. No disruption of the skin was evident.
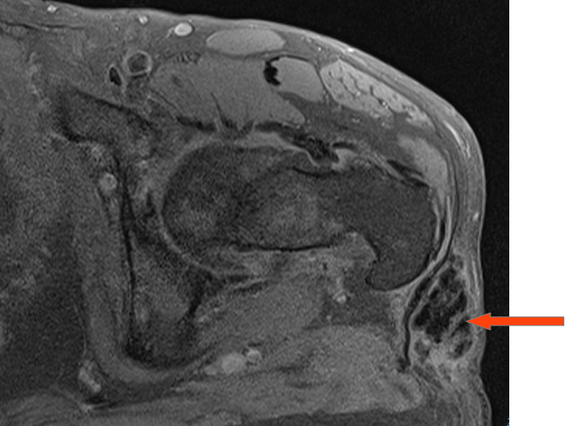
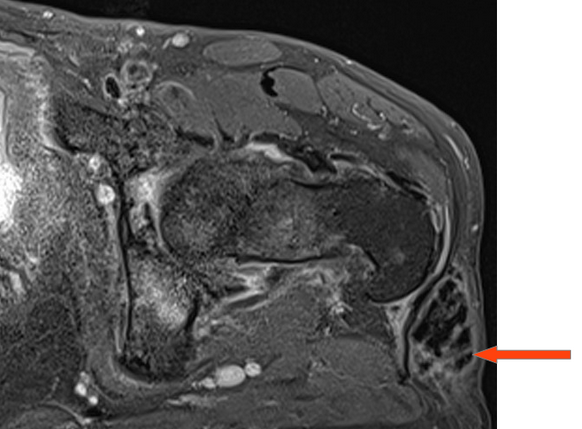
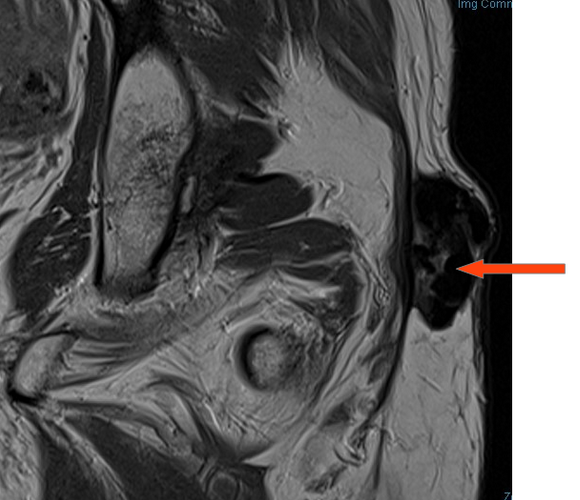
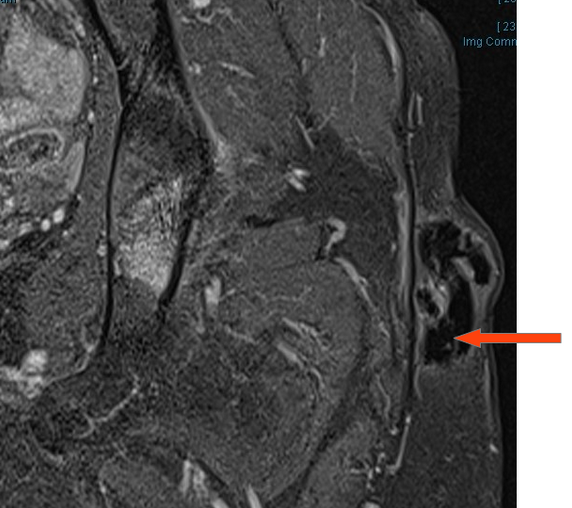
The patient presented to our department for MRI examination of this lesion. On MRI, there was a 4cm lobulated soft tissue mass in the subcutaneous tissues overlying the greater trochanter. This exhibited marked homogeneous low signal on all sequences. There was only peripheral linear enhancement on post-gadolinium sequences, and no significant internal enhancement.
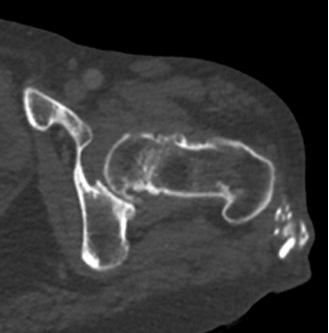
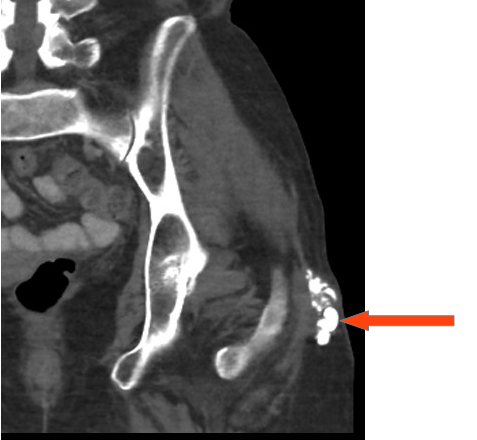
On review of an abdominal CT two years prior, there was a calcified solid subcutaneous lesion in this location, but smaller in size compared to the current study.
Soft tissue calcification can be seen in a number of conditions, some of which are aggressive in nature.
Differential diagnoses would include myositis ossificans, however there is no history of prior trauma, and typically chronic myositis ossificans appears as mature bone with cortex and medullary canal, unlike the appearance here.
There was some clinical concern for a sarcoma, however there are no solid enhancing components to support this diagnosis. Calcium hydroxyapatite deposition can have a similar appearance but tends to deposit in ligaments and tendons.
This lesion has appearances favouring tumoral calcinosis, a benign and rare familial condition characterised by large periarticular calcific masses caused by a hereditary metabolic dysfunction of phosphate regulation.
This case illustrates the need to combine clinical history with the imaging characteristics of a soft tissue lesion, both current and prior imaging, to help establish a diagnosis.
Figure 1: Frontal pelvic x-ray from 2 years prior showing a lobulated soft tissue mass overlying the left greater trochanter

Figures 2,3: axial and coronal CT from 2 years prior to current presentation showing homogeneous lobulated soft tissue mass in the subcutaneous tissues. Note that the calcification is amorphous and does not have the appearance of mature bone (with a dense outer cortex and internal medullary bone)
Figures 4,5,6: Axial precontrast and postcontrast T1 fat saturated images and axial T2 fat sat images through the lesion. There is lobulated homogeneously low signal in the mass, and no significant enhancement
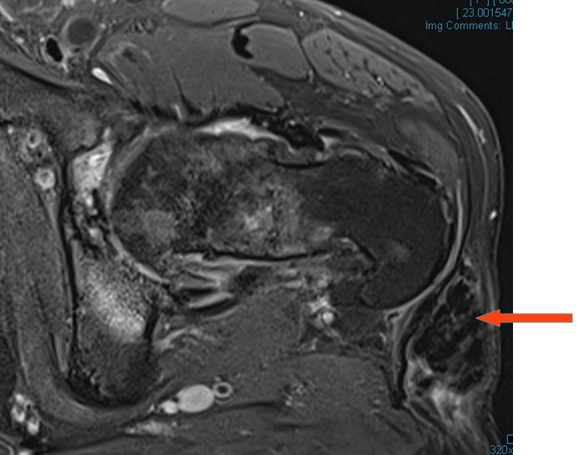
Figures 7,8: Coronal precontrast proton density and postcontrast T1 fat sat images
Dr Sebastian Fung is a musculoskeletal radiologist who undertook an MRI imaging fellowship in Hospital for Special Surgery in New York. He works in Sydney at St Vincent’s Private Hospital and Mater Hospital.
