Not all bone lesions with multiple bones involved are malignant.
A 49-year-old man presented severe medial sided pain in his right knee over a period of a few years on the background of weight gain. He reported pain medially more so than laterally on weightbearing, walking and climbing stairs. There was no antecedent history of trauma. He was otherwise well, with no history of a primary malignancy.
He was referred to have a radiograph and an MRI of his knee by a rheumatologist to investigate the cause of his symptoms.
On radiographs, there are numerous sclerotic (i.e. dense) foci within the medullary bone of the femur, tibia and fibula. These are well defined, exhibit a narrow zone of transition (i.e. sharp margins), with no evidence of periosteal reaction, cortical breakthrough, soft tissue mass or pathological fracture (these features generally pointing to aggressive bony lesions). Lesions are seen in the foot and hips in this same patient.
However, their multiplicity and polyostotic involvement (i.e. involvement of multiple bones) can be seen in either systemic metastasis or systemic bony conditions, most often developmental in nature. Note that some of the sclerotic lesions are almost linear in nature, parallel to the long axis of the bony trabeculae in the femur.
On MRI, this is further delineated, with well-delineated intramedullary lesions which are intensely and homogeneously low signal on all sequences. There is no associated marrow oedema, and no sinister features similar to the X-ray apart from multiplicity.
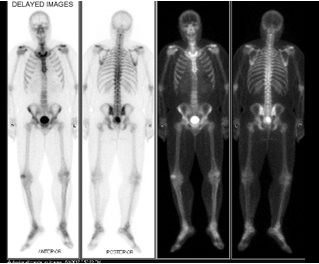
Another reassuring feature is that on nuclear medicine bone scan, there is no increased uptake of radiotracer (i.e. they are not “hot” on bone scan) indicating little in terms of osteoblastic activity. A differential diagnosis would be that of osteoblastic metastases particularly with primary neoplasms such as prostate cancer. However, a negative prostate specific antigen test and lack of uptake on bone scan would militate against this.
This constellation of findings is typical for a rare autosomal dominant bone dysplasia called osteopoikilosis, where there is a genetic defect resulting in numerous bone islands particularly centred around joints and typically having a morphology where they appear elongated along the long axis of the bone. The condition is asymptomatic and does not degenerate into malignancy. Bone strength is normal.
The teaching value of such a case is that not all bone lesions with multiple bones involved are malignant. Analysis of the imaging features, clinical history and laboratory markers can often yield a confident diagnosis, sparing the patient from unnecessary invasive investigations.
Figure A – Knee radiographs showing numerous sclerotic osseous lesions, some of which appear elongated along the long axis of the bones.
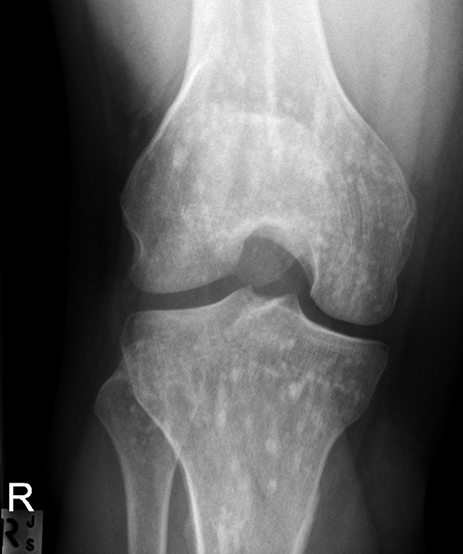

Figure B – Sagittal PD and T2 fat saturated MRI images demonstrating homogeneously low signal multiple bony lesions with no marrow oedema or sinister features.
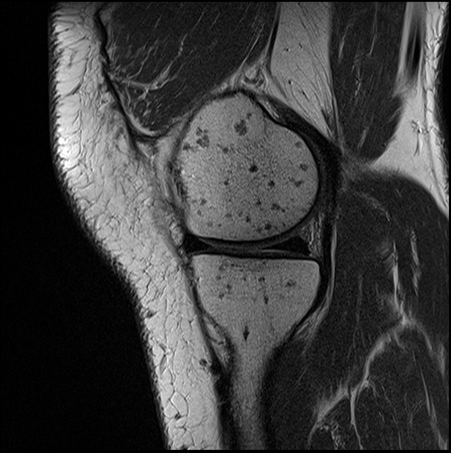
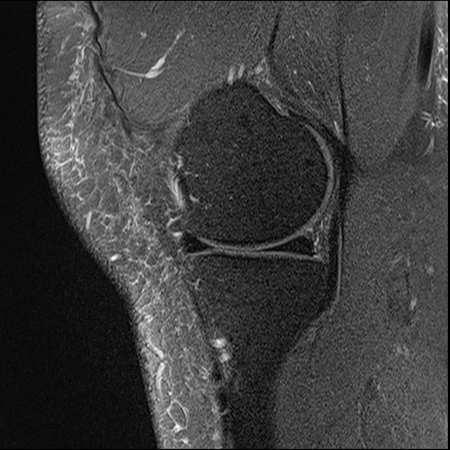
Figure C – Coronal PD image demonstrating elongated low signal lesions

Figure D: Radiograph of the hips and foot in the same patient showing similar sclerotic lesions


Figure E – nuclear medicine bone scan showing lack of radiotracer uptake in the skeleton.