

A support group for women rheumatologists is becoming more vocal about inequality in the profession, but some male specialists are confused (and a little offended) by the movement
While #notallmalerheumatologists are perplexed by the women in rheumatology movement in Australia, there is a distinct feeling of hurt and indignation among some male doctors.
It’s not that they’re against equal pay and representation for their female colleagues. Far from it. It is just difficult to accept that their specialty isn’t already sexism-free.
The general feeling is that rheumatology is different; it isn’t like other medical specialties.
There’s some truth in this. There are even numbers of male and female rheumatologists. Women are often leaders in the profession, accounting for five out of the nine ARA executive positions.
While no male rheumatologist would ever shout this from the rooftops, some are definitely wondering: Is this sudden burst of feminism in rheumatology just an unfortunate spill-over from the broader #metoo movement?
Is there actually a gender equality issue in rheumatology, or is the ARA’s Women in Rheumatology Australia (WIRA) special interest group just jumping at shadows?
WIRA’s founders have been quietly working on issues that affect women rheumatologists for years, but for those men who haven’t been involved, the arrival of feminism in rheumatology can feel a little confronting.
“You know, it’s sort of like a lot of males these days are totally on the back foot by the #metoo movement,” Dr Ann Leslie, a rheumatologist based in private practice in Sydney and the co-chair of WIRA, says.
“They are kind of thinking, ‘Oh my God, we can’t do anything now and we are under attack’, which is completely not the case.
“I have friends where I think, ‘Surely, I don’t have to explain this to you?’ But it takes some time to change perceptions and change attitudes and I suppose that’s why we’re going slowly with some of the more controversial things that we could be talking about.
“There are a lot of men who are in denial about the challenges faced by women in professions like rheumatology, where there is a long period of training involved before people make it to senior levels,” says Professor Matthew Brown, a clinician-scientist based in Queensland and the APLAR-ARA conference organiser who was instrumental in ensuring an even gender split in speakers this year.
“And so, it doesn’t surprise me that some people would be resistant [to a women in rheumatology group],” he says. “If you get a big enough group,
I think you’ll always get that diversity of opinion. But I don’t think it’s a majority opinion.”
HUMBLE ORIGINS
WIRA has become more vocal about gender inequity in recent years, but the group wasn’t focused on advocacy in the beginning.
“It started off very loosely several years ago with a group of friends saying, ‘We really should get together a bit more’,” says Dr Leslie.
This informal catch-up evolved into a professional support network and was folded into the Australian Rheumatology Association as a special interest group a few years ago.
“It’s still really in its early days,” says Dr Leslie. “But each year we are getting a better idea about what we want to achieve and how to go about doing it.”
Dr Leslie is a mother of four children who has been working part-time as a rheumatologist in Sydney for about three decades.
It helps to have a group that focuses specifically on women rheumatologists, she says. “Women do tend to gravitate more to women because, again, shared experiences and maybe a perception that there will be a better understanding of the kind of issues that they will face.”
In its formal terms of reference, WIRA says its purpose is “to support women in all aspects of rheumatology practice” through education, mentoring and encouraging women to take on leadership roles.
The group meets once a year at the ARA scientific conference. They also try to organise an annual dinner but, as rheumatologists and mothers, sometimes they’re all just too busy, says Dr Leslie.
Not all of WIRA’s members are signed up to WIRA’s email newsletter, but the email has a 50% open rate, which is “pretty good”, says Dr Leslie.
WIRA now sends its newsletter out with the ARA’s monthly newsletter, which means that all ARA members receive it, men and women.
WIRA is also now crossing international borders to connect with other women’s associations around the globe.
Dr Grace Wright, a New York rheumatologist and the President of the Association of Women in Rheumatology (AWIR), and her colleague Dr Gwenesta Melton, were recently invited to speak at WIRA’s meeting at APLAR-ARA in Brisbane in April. The American group is much larger than the Australian association, with chapters across 18 states.
“It was wonderful to hear of their work,” says Dr Leslie. “It was really inspiring. The American version is very much more formal and further down the track than us.
“It’s very well-established. They have a pretty vibrant social media where there are a lot of conversations, comments and discussion. They have a very professional website.”
The American group hosts its own national conference and educational events, sponsored by pharmaceutical companies.
The US group’s upcoming immunology bootcamp is supported by educational grants from AbbVie, Amgen, Bristol-Myers Squibb, Genentech, GlaxoSmithKline, Lilly, Merck, and Sanofi Genzyme and Regeneron Pharmaceuticals.
“I don’t think we will ever really aspire to in that way because there’s a lot of sponsorship money behind it, which is not a direction that we would really want to be going in at the moment,” says Dr Leslie. “But our goal and our aims and philosophies are very similar.”
IS RHEUMA GENDER EQUAL?
When it comes to demonstrating gender inequality in medicine, the numbers speak for themselves. While around half of doctors are women in Australia, only 12.5% of large hospitals have a female CEO and only 28% of medical schools have female deans.
In 1986, 16% of non-GP specialists were women. In 2015, this increased to 33%, so not much of an improvement there.
Men continue to dominate the field of surgery, with 94% of orthopaedic surgeons and 88% of cardiothoracic surgeons being male, according to the Australian Bureau of Statistics’ 2011 census.
However, there are a few specialties with a more even split. These include endocrinology (59% female), pathology (58% female) and paediatrics (53% female), and obstetrics and gynaecology (49% female).
There are 376 consultant rheumatologists in Australia (these are the full members of the ARA). Of these, 42% are women. Among trainee rheumatologists, there’s more likely to be a 50:50 male-to-female ratio.
So, if roughly half of rheumatologists are women, is rheumatology immune to gender inequality? The data, although limited so far, would suggest otherwise.
Take a look at the approximate proportion of female speakers at the ARA’s annual scientific meeting over the past five years:
2019 – 50% women, 50% men
2018 – 30% women, 70% men
2017 – 50% women, 50% men
2016 – 40% women, 60% men
2015 – 30% women, 70% men
“After we saw those statistics for 2018, we wrote to the board of the ARA highlighting that as an issue,” says Dr Helen Benham, a rheumatologist based in Queensland and the co-chair of WIRA. “And, on the back of that, we are very pleased that in 2019 it was 50:50.”
Professor Brown says men are almost always over-represented at international rheumatology conferences.
“There are few different possible reasons for that,” he says. “One is that the committees that actually design the conferences tend to be dominated by men and that there is a habit of basically inviting the ‘usual suspects’.”
Women didn’t get as many invitations to speak at conferences and therefore miss out on the career-advancement that this kind of recognition brought, says Professor Brown.
Academic titles such as professor and associate professor are still overwhelmingly bestowed upon male rheumatologists, he says.
To achieve a 50:50 gender split in speakers, Professor Brown and the other conference organisers made a point of inviting up-and’coming female rheumatologists because there were not enough women with prestigious titles to fill all the positions.
“So, in the end, we had somewhere around 110 invited speakers and there was a slight female majority.”
DOLLAR SIGNS
In Australia, female doctors have total earnings of about half of that of male doctors, according to data published by the Australian Taxation Office in 2016.
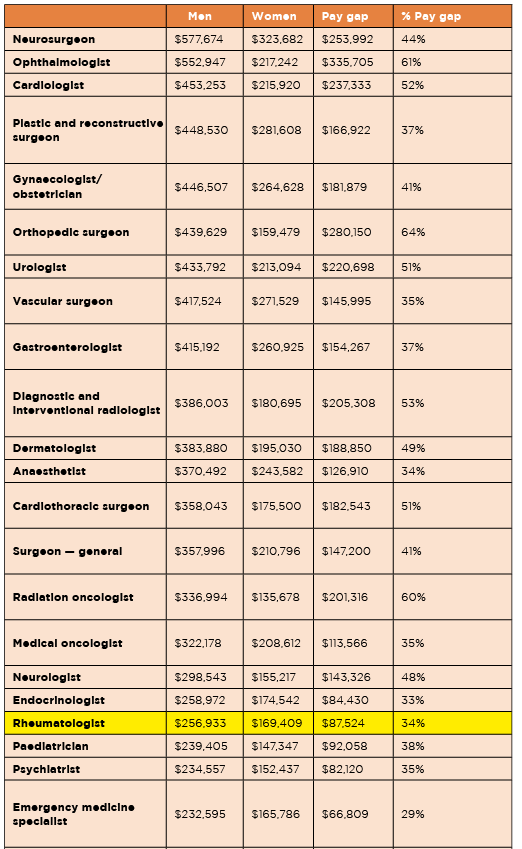
Across 22 of the top-paying medical specialties, in total female specialists earned on average 44% less than men.
“The most recent data shows that, on average, male rheumatologists earn $256,933 and female rheumatologists earn $169,409,” says Dr Benham.
“So, that’s a significant gender pay gap, which is actually, certainly not exclusive to rheumatology, but in fact present across many of the medical specialties.”
While some of this pay gap can be atttribited to female rheumatologists working fewer hours per week than theire male counterparts, that does not explain all of difference. When the figures are adjusted for working hours, female specialists still earn 16.6% less than male specialists, according to the AMA.
In rheumatology, the gap might be explained by women taking on more family caring responsibilities, doing more bulk billing and taking on less consultancy work than men, Dr Leslie says.
“At the moment, we are trying to get some accurate numbers just on the gender pay gap, for instance, and how much of our working hours are spend on family duties outside our work,” she says.
WIRA recently sent out a workforce survey through the ARA with questions on pay, family responsibilities, maternity leave and bullying and discrimination.
“We are still waiting on the ARA to present the results so we can’t comment on that data,” says Dr Benham.
SETTING GOALS
In the next 12 months, WIRA has set its sights on trying to improve flexible and part-time training, as well as promoting job-sharing arrangements, which will help rheumatologists work while raising a family.
The organisation is also working to support mentoring for women rheumatologists and is putting together a list of female speakers so that “there is no excuse for an absence of women in these roles”.
To help more women become confident speakers, WIRA will be calling on experienced presenters to help develop a workshop or short course on presentation skills for rheumatologists.
“The other issues, of course, are around childcare,” says Dr Benham.
APLAR-ARA’s organisers made a serious attempt to offer low-cost childcare at its conference centre this year, and even went as far as arranging sponsorship, but despite there appearing to be a lot of demand for the service, only one family registered to take up the offer.
Over the next year, WIRA will be advocating for childcare at all conferences, says Dr Benham.
MALE MEMBERSHIP
WIRA is very keen to engage with male rheumatologists and encourages men to sign up as members, says Dr Benham.
“Because many of these issues are, of course, family issues and issues that we would love everybody to be involved with,” says Dr Benham. “But we don’t shy away from the fact that, unfortunately, many of these issues affect women disproportionately.”
Dr Benham couldn’t recall seeing any men at the WIRA meeting this year, and only a few males have become members of WIRA.
Some men did come up to the WIRA stand at the APLAR-ARA conference to ask about the group, ”so that was really encouraging”, says Dr Benham.
“To be honest, I didn’t know that they actually invited men,” admits Professor Brown, who is not a member of WIRA. “I was always thought with the title that it is actually a women’s group. I’d be happy to join now that I know men are welcome.”
As a final question, The Medical Republic asks Dr Benham: Is it sexism or unconscious bias that is driving gender inequality in rheumatology?
“Hah, well, I mean there are lots of theories as to why gender inequity exists,” she replies.
“And, of course, it is impossible to say that, particularly in rheumatology, there is one thing or the other. So, what is a better strategy is actually find the issue, analyse the issue and then demonstrate to our whole membership the issue that exists, so that we can collectively all address it.”
