The COVID-19 pandemic in the United States has been associated not only with tens of thousands of excess deaths from COVID-19 but also from other non-respiratory causes, research suggests.
Welcome to The Medical Republic‘s live COVID-19 blog.
Got any tips, comments or feedback? Email me at bianca@biancanogrady.com
The latest
- Afternoon update: Excess deaths seen from non-respiratory causes in US during COVID-19, and advice on managing patients with Cushing’s syndrome during the pandemic.
- Morning update: More healthcare workers diagnosed with COVID-19 in Victoria, study highlights major weaknesses in evidence for serological SARS-CoV-2 tests, and Australian company launches first southern hemisphere vaccine trials.
- The COVID-19 pandemic in the United States has been associated not only with tens of thousands of excess deaths from COVID-19 but also from other non-respiratory causes, research suggests.
Writing in JAMA, researchers reported that from 1 March to 25 April, around 87,000 excess deaths – the difference between observed and expected deaths – were reported, from a total of 505,000, of which 65% were attributed directly to COVID-19.
However in many states, more than half of these excess deaths were from causes other than COVID-19, and the five states with the highest number of COVID-19 deaths also showed the largest proportional increases in these non-respiratory deaths. In these states, deaths from diabetes increased by 96%, deaths from heart disease by 89%, deaths from Alzheimer’s disease increased by 64% and deaths from cerebrovascular disease increased by 35%.
New York City showed the highest increases in non-respiratory deaths during this period, with deaths from heart disease increasing nearly four-fold.
“Further investigation is required to determine the extent to which these trends represent nonrespiratory manifestations of COVID-19 or secondary pandemic mortality caused by disruptions in society that diminished or delayed access to health care and the social determinants of health (eg, jobs, income, food security),” the authors wrote. - Patients with active Cushing’s syndrome may present with different COVID-19 symptoms – such as less fever or breathing difficulties – so clinicians should look at a broader array of symptoms, according to a comment published in The Lancet Diabetes & Endocrinology.
Up to half of patients with Cushing’s syndrome have an increased risk of infection due to a compromised immune system, the authors wrote. While there have not yet been COVID-19 studies done in this patient population, they suggested that some of the more common symptoms of COVID-19 – such as fever and cough – may be less pronounced in patients with Cushing’s.
“Therefore, during active Cushing’s syndrome, physicians should seek different signs and symptoms when suspecting COVID-19, such as cough, together with dysgeusia, anosmia, and diarrhoea, and should be suspicious of any change in health status of their patients with Cushing’s syndrome, rather than relying on fever and dyspnoea as typical features,” they wrote.
They also highlighted impaired glucose metabolism and hypertension as two negative prognostic factors, and stressed the importance of optimising blood glucose and blood pressure control in these patients.
- A study published in the BMJ has cast doubt on the diagnostic accuracy of SARS-CoV-2 serological tests and argued there are ‘major weaknesses’ in the evidence base for these tests.
An international team of researchers has conducted a systematic review and meta-analysis of 40 studies of SARS-CoV-2 serological tests, and found that half weren’t peer-reviewed, only 10% involved outpatient populations, and only 45% stratified the sensitivity of the tests by time since the onset of symptoms. Of the 17 tests that evaluated point-of-care tests, only two actually tested them at point-of-care.
The analysis also found that 98% of studies showed high or unclear risk of bias in their patient selection, and many studies weren’t clear about aspects such as whether the cut-off values for positive, negative or indeterminate were pre-specified.
When comparing different methods, the authors found that lateral flow immunoassays had consistently lower sensitivity than other methods such as enzyme linked immunosorbent assays (ELISA) or immunoglobulin assays for antibodies.
“These observations indicate important weaknesses in the evidence on covid-19 serological tests, particularly those being marketed as point-of-care tests,” the authors concluded. “Overall, the poor performance of existing serological tests for covid-19 raises questions about the utility of using such methods for medical decision making, particularly given time and effort required to do these tests and the challenging workloads many clinics are facing.” - An Australian biopharmaceutical company is the first to launch human trials of a COVID-19 vaccine in the southern hemisphere.
Vaxine Pty Ltd has announced it is commencing phase 1 trials of its vaccine at the Royal Adelaide Hospital, which will involve 40 healthy individuals given either the vaccine or placebo to monitor protective antibody and T-cell responses. The vaccine targets the spike protein on SARS-CoV-2. - Victoria’s COVID-19 case numbers continue to increase, with several new outbreaks reported, including two healthcare workers – one at the Joan Kirner Women’s and Children’s Hospital, and Epworth. Three students at separate schools have also tested positive, as well as two cases at an early learning centre. New South Wales recorded 14 new cases yesterday, all in returned travellers in hotel quarantine.
Meanwhile, Australia’s total COVID-19 test count has topped 2.5 million, and nearly 50,000 tests have been conducted in the last 24 hours alone.
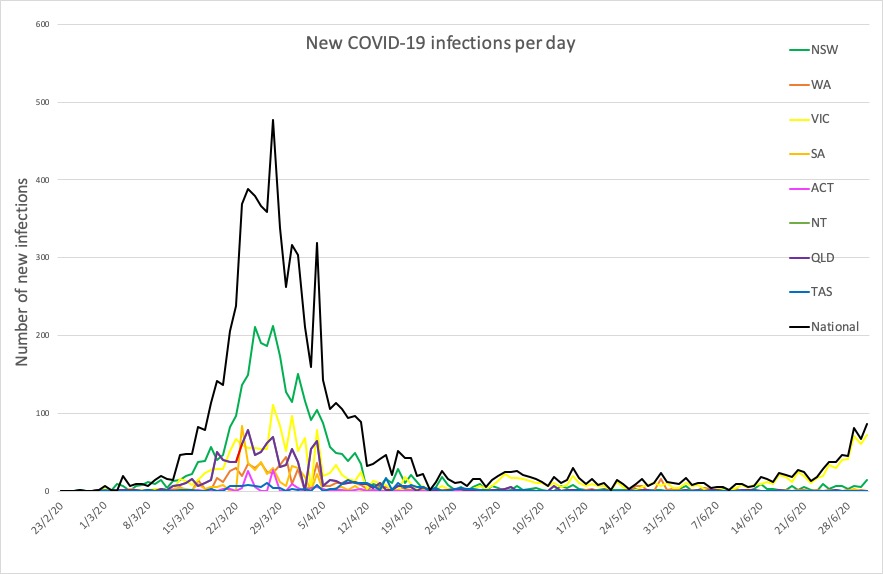
Around Australia to 9pm yesterday, here are the latest confirmed COVID-19 figures:
National – 7920, with 104 deaths and 7063 recovered
ACT – 108
NSW – 3203
NT – 29
QLD – 1067
SA – 443
TAS – 228
VIC – 2231
WA – 611