Results from a phase 1/2 randomised controlled trial of a SARS-CoV-2 vaccine suggest safety and immunogenicity.
Welcome to The Medical Republic‘s COVID Catch-Up.
It’s the day’s COVID-19 news into one convenient post. Got any tips, comments or feedback? Email me at bianca@biancanogrady.com.
21 July
- New vaccine results suggest safety and immunogenicity.
- Deaths from cancer likely to increase due to delayed diagnosis from pandemic shutdowns, study suggests.
- Influenza rates drop by more than 75% in Singapore during pandemic.
- Thrombosis and hypercoagulability an issue in severe COVID-19.
- NSW warns against non-essential travel and large gatherings as more outbreaks occur.
- The buzz today is all about the latest COVID-19 vaccine news. Results from a phase 1/2 randomised controlled trial of a SARS-CoV-2 vaccine are making all the right immunological noises, but with the great big caveat that researchers don’t yet know if it will work.
The ‘Oxford vaccine’ – aka ChAdOx1 – consists of a non-replicating viral vector engineered to express the SARS-CoV-2 spike protein on its surface. In the study published in The Lancet, researchers tested the vaccine in 1078 healthy volunteers (not all heroes wear capes) – half of whom got the SARS-CoV-2 vaccine and half of whom got a meningococcal conjugate vaccine as a comparable antiviral vaccine control.
The first bit of good news was that the vaccine appeared to be fairly safe, with fatigue and headache the most common systemic reactions. Most participants experienced some localised pain and tenderness at the injection site, but both the systemic and local reactions were reduced in individuals who were given paracetamol before they were immunised.
The vaccine also appeared to induce significant levels of neutralising antibodies against the SARS-CoV-2 spike protein in all participants, and these reached levels capable of neutralising live virus within 28 days of the vaccine being administered. The amount of neutralising antibodies was higher in the participants who were given two doses of the vaccine instead of one.
The next steps are to move to phase 2 and 3 trials in larger and more diverse populations, including older people with comorbidities, and children. And most importantly, the current – and future – study populations will be followed up to see if any of them contract COVID-19. There’s still a long way to go. - Deaths from breast cancer are likely to increase by 8% or more in the five years after diagnosis, as pandemic lockdowns in the UK contribute to a delay in diagnosis, a study has estimated.
The paper, published in The Lancet Oncology, also estimated that colorectal cancer deaths will increase by around 16%, lung cancer deaths by around 5%, and oesophageal cancer deaths by around 6%.
The authors used population data on these four cancers to estimate the impact of diagnostic delays, up to five years after the diagnosis was made, on the diagnostic pathway of individuals, on their survival, and therefore on excess mortality at a population level.
Overall, they calculated an additional 59,000 to 63 000 years of life lost to cancer could be attributed to delayed diagnoses during the COVID-19 lockdown. - Some good news: Singapore has seen a 76% drop in the estimated daily number of influenza cases during the peak of the COVID-19 pandemic and lockdowns, compared to the same period in previous years. Writing in Emerging Infectious Diseases, the authors noted that public health efforts to control the spread of COVID-19 have likely reduced the spread of influenza.
- The role of hypercoagulability and thrombosis in severe COVID-19 has been further illuminated by two studies published yesterday; one finding more than 29% of intensive care patients with COVID-19 have a thrombotic event – which is associated with higher mortality – and another reporting on three patients with pulmonary emboli and elevated D-dimer levels.
The first study, published in JAMA, looked at more than 3300 consecutive patients hospitalised with severe COVID-19 in New York, nearly 14% of whom experienced a venous thrombotic event and nearly 19% experienced an arterial thrombotic event. The overall rate of thrombotic events was nearly 30% in those in intensive care and just over 11% in those not in intensive care. Any thrombotic event was associated with 82% greater risk of death, but most patients in the study were treated with prophylactic low-dose anticoagulants.
The second study, published in Emerging Infectious Diseases, reported on three cases of patients admitted to intensive care with COVID-19 in the US, who all developed pulmonary emboli despite DVT prophylaxis. All three showed high levels of D-dimer on admission – one recorded 33,318 ug/mL – and two patients had increases in D-dimer levels over the course of their illness.
The authors noted that pulmonary emboli can occur after the cytokine storm in COVID-19, even in those given DVT prophylaxis. “Monitoring disseminated intravascular coagulation and measurement of platelet counts, d-dimer and fibrinogen levels, and trending International Society of Thrombosis and Haemostasis scores might be beneficial for early diagnosis of PE in patients with COVID-19,” they wrote. - COVID-19 has claimed three more lives overnight in Victoria, including that of a centenarian, according to Premier Dan Andrews’ latest press conference.
The requirement to wear a face masks in metropolitan Melbourne and Mitchell shire will be enforced from midnight on Thursday 23 July, with the delay intended to give people time to buy or make a face covering.
There are some exemptions to the mask rule: children under 12, people with a medical or professional reason not to wear one, or if it’s not practical, such as when going for a run.
In NSW, health authorities have called for anyone who attended religious services at the Our Lady of Lebanon Cathedral in Harris Park, western Sydney, on the 15, 16 or 17 of July to self-isolate and get tested. A positive case associated with the Thai Rock outbreak attended a service on those days, and two parishioners have since tested positive.
NSW Health said in a statement that although it was not (yet) a legal requirement, “it would be preferable and safer for the time being to avoid all non-essential travel, and not host or attend gatherings of more than 10 people at home.” They singled out hotels, restaurants, gyms and social gatherings as situations where people should exercise particular caution.
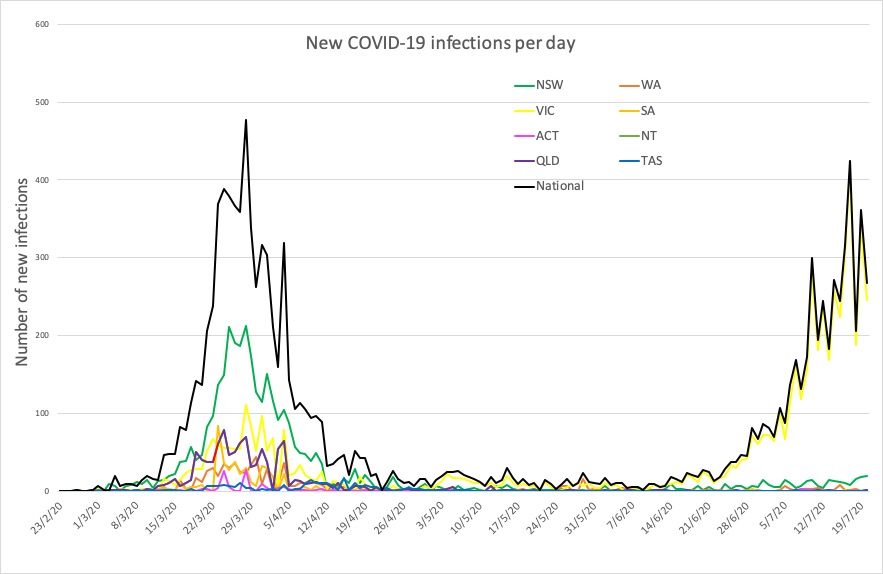
Here are today’s confirmed COVID-19 infection figures from around Australia:
National – 12,069, with 123 deaths and 156 hospitalised.
ACT – 113
NSW – 3588
NT – 31
QLD – 1072
SA – 444
TAS – 228
VIC – 5942
WA – 651