

Despite all the enthusiasm about remdesivir in the US, the Australian National COVID-19 Clinical Evidence Taskforce is taking a more cautious line
Thanks for spending this week with us on The Medical Republic‘s live COVID-19 blog.
And thank you to our sponsor and supporter for funding this project with an independent grant, Boehringer Ingelheim.
The latest
- Australia’s taskforce on COVID-19 clinical evidence reiterates that remdesivir is for clinical trial use only.
- More evidence for an animal – not a laboratory – origin for SARS-CoV-2.
- Elective surgery to resume, says PM.
- Despite all the enthusiasm about remdesivir in the United States, the Australian National COVID-19 Clinical Evidence Taskforce is taking a more cautious line, advising that the antiviral drug – and other experimental treatments for COVID-19 – should only be used in the context of a clinical trial.
In what might be an oblique comment on the as-yet incomplete release of data on remdesivir study conducted by the National Institutes of Health, taskforce Chair Associate Professor Julian Elliott said in a statement that, “getting the best possible care does not mean trying a medicine that is getting a lot of buzz on social media.”
The latest update to the ‘living guidelines’ on COVID-19 includes new recommendations favouring the use of videolaryngoscopy over direct laryngoscopy in adults with COVID-19 who are undergoing endotracheal intubation, as well as recommendations on higher versus lower positive end-expiratory pressure (PEEP) for mechanically ventilated patients, and on the continuation of ACE inhibitors and ARBs in patients with hypertension and COVID-19. - And to leave you this Friday afternoon with something a bit lighter, here’s another gem from US comedian Sarah Cooper, lip-synching to Trump’s latest ramblings. Content warning: this one will give the public health folks a stroke.
How to more cases than anybody in the world pic.twitter.com/VA9bPJiQ6i
— Sarah Cooper (@sarahcpr) May 15, 2020
- Pangolins and bats and cats, oh my! The weight of evidence in favour of an animal origin of COVID-19 just got a little weightier (sorry, conspiracy theorists and governments wanting to pick a fight ) with the discovery of a SARS-CoV-2-like virus in bats.
Writing in Current Biology, a team of Australian and Chinese researchers report their discovery of a new bat-derived coronavirus – called RmYN02 – which is 93.3% genetically-identical to SARS-CoV-2, making it the closest relative of SARS-CoV-2 found so far.
Their sequencing suggests that this bat virus may not use the ACE2 enzyme to access human cells, as SARS-CoV-2 does. But it does show the same sort of changes to the genome of the spike protein – the protein that SARS uses to gain access to cells – suggesting that these changes can occur naturally in this group of viruses rather than being the result of engineering.
- Elective surgery is back on the menu. In his weekly post-National Cabinet meeting press conference today, the Prime Minister announced the resumption of elective surgery but left the details up to individual states.
According to the Guardian, Chief Medical Officer Professor Brendan Murphy followed the announcement by pointing out that there were now only 50 COVID-19 patients in hospitals around the country, and 12 on ventilators, but hospitals were only at around 50%-60% capacity.
The PM also announced that the national cabinet had given the go-ahead to a $48 million national mental health and wellbeing pandemic response plan.
- The similarities between recovery from severe COVID-19 and recovery from sepsis has prompted the UK Sepsis Trust to reissue its booklet for patients leaving a critical care unit after serious illness, but tailored for COVID-19 survivors.
“People are often shocked and upset by what someone in Critical Care has gone through,” the booklet notes. “This may have been made worse if this was due to CoVID-19 because of the visiting restrictions – people might not have seen quite how ill you were, so it’s easy to understand why they might expect you to feel better very soon.”
The booklet covers everything from recovery times, what treatment they may have received in critical care, how patients may be feeling and thinking after discharge, and what they can do to help their recovery.
Interviewed in the British Medical Journal, intensive care specialist, founder and CEO of the UK Sepsis Trust Dr Ron Daniels said the recovery profile from COVID-19 was similar to that of sepsis, and there was evidence that survivors would have significant ongoing rehabilitation needs, particularly in the neurocognitive and neuropsychiatric domains.
- How do you handle a COVID-19 patient without getting infected yourself? Just put a BADGER on their head.
The BADGER – Box for Aerosol and Droplet Guarding and Evacuation in Respiratory infection – is the brainchild of a bunch of clinicians and researchers in the United States who wanted to develop a transparent, semi-sealed device that could contain any infectious droplets or aerosol particles from infected patients but still allow clinicians to perform tasks such as intubation.
What they came up with – and reported in the non-peer-reviewed preprint server MedRxiv – looks like a miniature version of the glove boxes used to handle specimens in biosecure laboratories, that fits over a patient’s head as they are lying down, and has drapes to maintain a seal around the neck and shoulders.
It’s supposed to be connected to in-wall vacuum suction to ensure negative pressure and constant airflow, and has multiple hand ports so clinicians can do what they need to do using the built-in gloves.
They did actually test how good the box was at preventing aerosol escape by nebulising a non-toxic bitter chemical inside the box and then seeing if anyone could smell it outside the box. Success! They even put a mannequin in there, along with smoke, and administered chest compressions on the mannequin to simulate coughing. Still, no smoke escaped.
But does it work on humans? The researchers got approval for clinical use from their university, and were able to successfully intubate and extubate patients who were being anaesthetised for surgery.
“As there is more evidence of aerosolized SARS-CoV-2 from innocuous activities such as sneezing and coughing, and current standard PPE might not fully prevent exposure for healthcare providers, the BADGER might be an additional layer of protection to mitigate airborne transmission of COVID-19,” they wrote.
- The term ‘hot-spot’ gets thrown around a lot in this pandemic, but what does it actually mean? In Australia, the definition of a COVID-19 hot-spot has actually been revised recently; it used to be defined as a Local Government Area with 60 or more confirmed cases in the previous two weeks. Now, just ten or more cases qualifies a location as being a hot-spot.
Now you know.
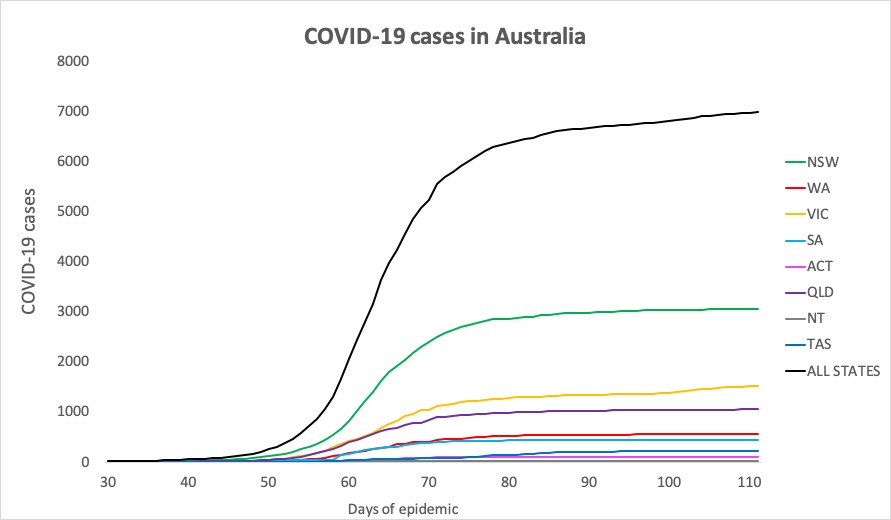
- We’re creeping ever-closer to the 7000 infections mark, which isn’t a milestone to celebrate but it could certainly be a heck of a lot worse. Here are Australia’s confirmed COVID-19 infections, to 9pm yesterday:
National – 6989, with 998 deaths and 6301 recovered
ACT – 107
NSW – 3063
NT – 29
QLD – 1052
SA – 439
TAS – 227
VIC – 1520
WA – 552
Disclaimer: The content on the Medical Republic COVID-19 blog is independently created by Medical Republic without input from Boehringer Ingelheim Pty Ltd. The views, information, or opinions expressed on the Medical Republic COVID-19 blog are Medical Republic’s own and do not necessarily represent those of Boehringer Ingelheim Pty Ltd. Boehringer Ingelheim Pty Ltd is not responsible for and does not verify the accuracy of any content on the Medical Republic COVID-19 blog.
